

Background: When it comes to aesthetic augmentation of the arms the upper arm is almost almost always what is done. The biceps and triceps of the upper arms are larger muscles in which subfascial and submuscular implant augmentation is possible and there are standard implant styles available to do so. When it comes to the lower arm, however, augmentation is much more of a rare procedure.
The forearm muscles are smaller, no standard implants exist for them and the patient requests are infrequent. Three types of forearm implant augmentations exist in my experience. The first type is for the muscular look so the size of the forearm better matches the larger upper arms. This is usually accomplished by augmentation of one of the largest muscles of the forearm, the brachioradialis in the upper lateral forearm. The second type is for patients who feel their forearms are too thin which usually refers to closer to the wrists or lower half of the forearm. Such augmentations do not follow any specific muscle group and are broader subcutaneous implants down to the wrist level. The third type is for patients with a motor nerve injury that have suffered muscle atrophy in one arm and the goal is improved forearm symmetry. These can involve multiple muscle areas depending on the ulnar or median nerve branch involvement. It is possible, but very rare, that a forearm augmentation patient may actually be a mixture of two types….augmentation and asymmetry correction.
Case Study: This male had a prior history of multiple aesthetic body implants of the trapezius, deltoids, pectoral, bicep and tricep implants. During one of his bicep implant procedures he suffered a partial radial nerve injury result in some partial atrophy of the brachioradialis (BRD) and extensor carpi radialis longus (ECRL) muscles of his right forearm.

 Under general anesthesia he underwent multiple upper extremity and shoulder implants which included forearm implants. Initially bilateral larger upper forearm implants for BRD muscle augmentation. The implants were placed under the fascia through a small skin incision lateral to the antecubital fossa.
Under general anesthesia he underwent multiple upper extremity and shoulder implants which included forearm implants. Initially bilateral larger upper forearm implants for BRD muscle augmentation. The implants were placed under the fascia through a small skin incision lateral to the antecubital fossa.

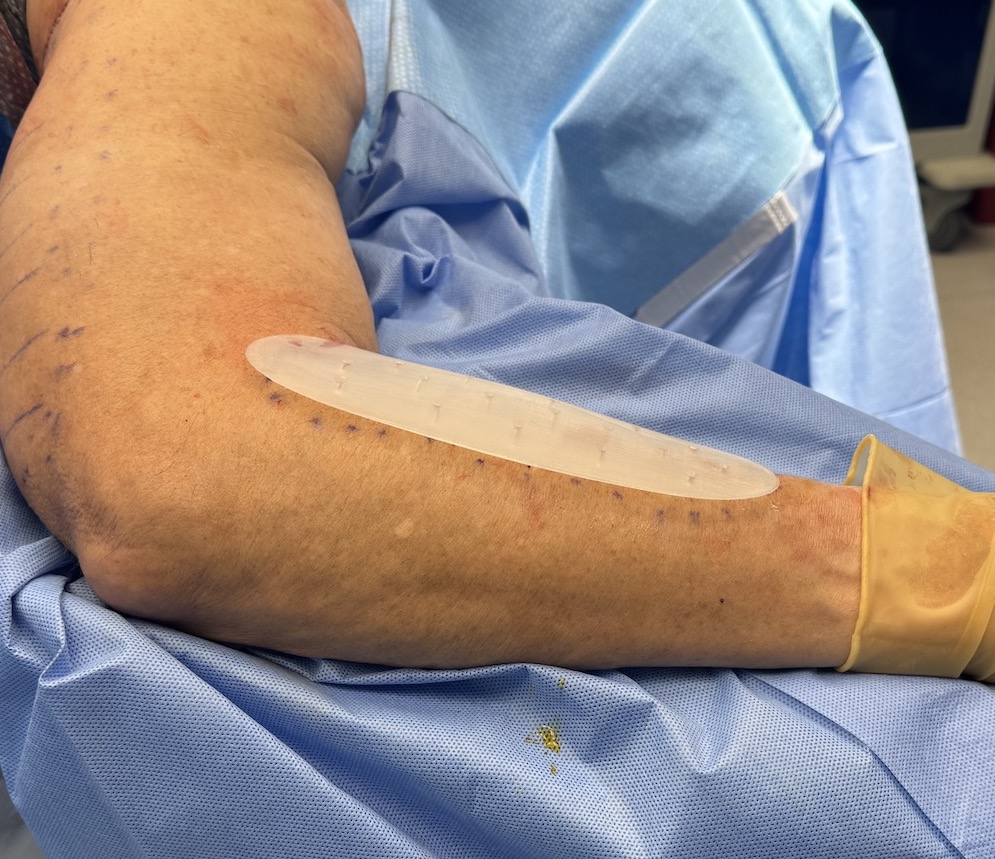
 In the right volar forearm an ultrasoft gummy bear feeling implant in shape of a long thin muscle was placed though a small incision at the mid portion of the implant.
In the right volar forearm an ultrasoft gummy bear feeling implant in shape of a long thin muscle was placed though a small incision at the mid portion of the implant.



 His short term forearm implant result was encouraging but there was some unacceptable implant edges along some of the implants. There were subsequently replaced with softer feather-edged implants that resolved the edging.
His short term forearm implant result was encouraging but there was some unacceptable implant edges along some of the implants. There were subsequently replaced with softer feather-edged implants that resolved the edging.

 The volar forearm implant was a bit prominent but it looked like a muscle so it was an acceptable result. His forearm symmetry was improved, not perfect, but improved with fuller upper forearms.
The volar forearm implant was a bit prominent but it looked like a muscle so it was an acceptable result. His forearm symmetry was improved, not perfect, but improved with fuller upper forearms.
Forearm implant augmentation can be successful but the thinner subcutaneous tissue layer requires implants that have very thin edges to avoid implant show. Since there are no standard style forearm implants and they have to be custom made the opportiunity for such implant designs exist.
Key Points:
1) The lower half of the arm (forearm) can have implant augmentation but not in a submuscular fashion.
2) The brachioradialis muscle area is the most common forearm implantation area but other forearm areas can be augmented as well.
3) The volar aspect of the forearm, which its more of a concavity than convexity can be augmented but with a different shape of implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon