


Background: Macrotia is present when the patient feels that their ear is too big. This is not just when a large earlobe is present, which is the most common reason patients may feel their ear is overly large, but when the entire ear from top to bottom is large. There are measurements which usually align with the patients perception and, as a general rule, when the ear is greater than 60 to 65mms in height, most will perceive it as being a big ear.
 Macrotia surgery for shortening the vertically long ear is typically done through reduction of the upper and lower thirds. The non-cartilage containing earlobe is the easiest to reduce as it contains no cartilage. The inferior helical rim technique shortens the earlobe while keeping the scar line in a largely hidden location. The upper third of the ear is reduced by a scaphal flap technique where the widened distance between the upper helical rim and the anti helical fold serves as the excision site. A back cut/excision of the helical rim in the middle third of the ear serves as the amount that the upper third of the ear will be shortened as the flap rotates downward.
Macrotia surgery for shortening the vertically long ear is typically done through reduction of the upper and lower thirds. The non-cartilage containing earlobe is the easiest to reduce as it contains no cartilage. The inferior helical rim technique shortens the earlobe while keeping the scar line in a largely hidden location. The upper third of the ear is reduced by a scaphal flap technique where the widened distance between the upper helical rim and the anti helical fold serves as the excision site. A back cut/excision of the helical rim in the middle third of the ear serves as the amount that the upper third of the ear will be shortened as the flap rotates downward.
While the traditional macrotia reduction approach works for many patients, there are some where the remaining size of the untouched concha may look disproportionate. Usually the upper and lower thirds of the ear are are proportionately larger than the concha and the traditional approach brings them into a better overall balance. But for those larger concha macrotia patients an alternative approach is to do the ear reduction centrally.
 Case Study: This female had been bothered her whole life by the large size of her ears. She never went out without having them covered, usually by her hair. The vertical length of her ears were 75mms. While all three thirds of her ear were large, the upper third and the middle concha were the primary contributors with the earlobe length having a more minor contribution. Her goal was maximum reduction and she wanted the large concha addressed. Scars were not a concern to her.
Case Study: This female had been bothered her whole life by the large size of her ears. She never went out without having them covered, usually by her hair. The vertical length of her ears were 75mms. While all three thirds of her ear were large, the upper third and the middle concha were the primary contributors with the earlobe length having a more minor contribution. Her goal was maximum reduction and she wanted the large concha addressed. Scars were not a concern to her.

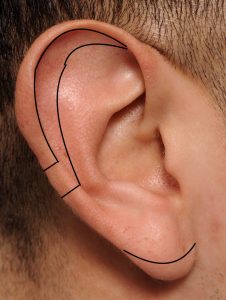
 Under local anesthesia a middle third resection pattern was marked with a stair step line across the helical rim onto the antihelix. Inside the lateral concha a crescent pattern was marked.
Under local anesthesia a middle third resection pattern was marked with a stair step line across the helical rim onto the antihelix. Inside the lateral concha a crescent pattern was marked.

 The resection was full thickness, including outer and inner skin and the intervening cartilage. The ear was then vertically shortened by bring down the upper third of the ear to close the created central defect as all three layers were put back together. In doing so it was not necessary to extend any scar lines onto the visible concha. As was anticipated bringing down the upper part of the ear created a forward bend to it which was fixed by a horizontal mattress cartilage suture through a small incision on its posterior surface. A helical rim earlobe reduction was done to complete the full vertical ear reduction.
The resection was full thickness, including outer and inner skin and the intervening cartilage. The ear was then vertically shortened by bring down the upper third of the ear to close the created central defect as all three layers were put back together. In doing so it was not necessary to extend any scar lines onto the visible concha. As was anticipated bringing down the upper part of the ear created a forward bend to it which was fixed by a horizontal mattress cartilage suture through a small incision on its posterior surface. A helical rim earlobe reduction was done to complete the full vertical ear reduction.



 On the opposite left side the exact same approach was used, bringing the ear height from 75mm to 55mms.
On the opposite left side the exact same approach was used, bringing the ear height from 75mm to 55mms.
There are several key points about the central wedge reduction macrotia surgery approach:
- 1) It does create a longer scar in the middle third of the ear than the traditional vertical ear reduction approach as it crosses both the helical and antihelical areas. So it should be reserved for those patients that have a large conchal bowl appearance.
- Because it leaves the upper third of the ear shape alone a larger scaphal area will remain. This is somewhat mitigated by the suture setback but it is the aesthetic tradeoff for addressing the large concha. It can also be reduced on its own in a secondary procedure if the patient desires.
- Because it can still be combined with an earlobe reduction, maximal vertical ear shortening is obtained.
- As is commonly perceived it is not necessary in making the concha look smaller to excise onto its more visible deeper bowl area. The lowered crus and antihelical fold areas, like a drawn pursestring, help close down its size.
Case Highlights:
1) Macrotia or a vertically long ear generally exceeds 60mms in a female.
2) The traditional technique in macrotia reduction is as top and bottom approach leaving the conceal bowl alone.
3) The central wedge technique is for the macrotia patient where the top and bottom approach would leave a disproportionately large appearing conchal concavity.
Dr. Barry Eppley
Indianapolis, Indiana