


Background: Reduction of broad or wide cheeks can only be effectively done by an osteotomy/bone repositioning technique. There is a very limited use of any cheek reduction by bone shaving as it does not remove enough bone and can not remove it where the real cause of cheek widening is.
The cheekbone is comprised of a major body of bone anteriorly (zygomatic major) and thin span of bone extending posteriorly which attaches to the temporal bone. This arch of bone exists to allow the temporal muscle to pass underneath it to insert onto the coronoid process of the mandible. This arch of bone is a major contributor to cheek width as it can have a flat or very convex shape to it. It is the zygomatic arch which is moved in by osteotomies by cutting it at both ends of its bony attachments, allowing the arch to move inward and reducing cheek width.
There have been numerous techniques to perform the anterior osteotomy through the larger zygomatic body from oblique to L-shaped bone cuts. The intraoral access allows good visualization to allow for the variety of different osteotomy line cuts. The posterior zygomatic arch, however, is very different. It is a thin rod of bone and only one osteotomy pattern can be made through it…a straight line cut. It also differs in terms of surgical access which typically requires a direct incision over it in the preauricular area.
In the male with beard skin the posterior zygomatic arch incision is at backside of the sideburn hair. But in the female with no sideburn or prominent preauricular tuft of hair the direct incision over the posterior zygomatic arch will leave a small bit visible scar. As a result a less visible scar approach is a preauricular incision (aka facelift approach)…which is convenient to use of the patient has already had facelift surgery.

 Case Study: This female desired reduction of her wide cheeks. She had prior double jaw surgery. (LeFort I impaction and sagittal split osteotomy)
Case Study: This female desired reduction of her wide cheeks. She had prior double jaw surgery. (LeFort I impaction and sagittal split osteotomy)

 Under general anesthesia and through an intraoral approach an oblique osteotomy cut was made with a reciprocating saw from the anterior end of the zygomatic body up to its junction with the lateral orbital rim. The anterior arch/cheek was infractured 6mms and secured with a 1.5mm plate and screws. The anterior edge of the medial cheekbone was shaved down to make it smooth with the infractured segment.
Under general anesthesia and through an intraoral approach an oblique osteotomy cut was made with a reciprocating saw from the anterior end of the zygomatic body up to its junction with the lateral orbital rim. The anterior arch/cheek was infractured 6mms and secured with a 1.5mm plate and screws. The anterior edge of the medial cheekbone was shaved down to make it smooth with the infractured segment.

 Through an existing facelift preauricular scar the end of the zygomatic arch was exposed by blunt dissection through a narrow opening. An osteotomy as used to make an oblique osteotomy cut which allowed its cut end to be pushed below and under the temporal end of the remaining arch. No plate fixation was used.
Through an existing facelift preauricular scar the end of the zygomatic arch was exposed by blunt dissection through a narrow opening. An osteotomy as used to make an oblique osteotomy cut which allowed its cut end to be pushed below and under the temporal end of the remaining arch. No plate fixation was used.
.
The incision was then closed with small resorbable sutures.
 In comparing the completed left side before the right side was done the effects of the cheekbone reduction could be seen.
In comparing the completed left side before the right side was done the effects of the cheekbone reduction could be seen.
 .
.
A postop 3D CT scan showed the anterior and posterior osteotomy cut lines.
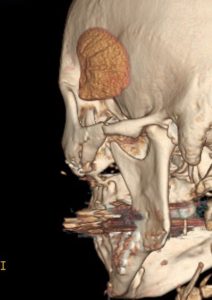 The inward movement of the posterior zygomatic arch could be appreciated in the scan from its posterior views.
The inward movement of the posterior zygomatic arch could be appreciated in the scan from its posterior views.
The posterior arch osteotomy, no matter the incisional approach, always is performed in an area where the frontal branch of the facial nerve runs very close by. The facelift incision does not avoid that risk any better than a direct incision but at pasty it avoids a visible skin scar.
Key Points
1) Cheekbone reduction is most effectively done with inward bone positioning using anterior and posterior osteotomies.
2) The anterior zygomatic body osteotomy is performed intraorally and can be done using various bone cut patterns with a reciprocating saw and small plate fixation.
3) The posterior zygomatic arch osteotomy can be done using a preauricular incision with an osteotome without plate fixation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon