

Background: An inadequate chin augmentation result can occur from a variety of factors. But chin implant removal in the treatment of an unsatisfactory chin augmentation result induces a whole new set of potential chin problems that now involve more than just a bony projection deficiency. The onset of undesired soft tissue changes (chin pad sagging, tightness and lower lip incompetence) creates a whole new set of problems that can become more challenging to treat than what motivated the patient to have the surgery initially.
When replacing chin implant with a sliding genioplasty the exchange should be reasonably similar in the amount of horizontal projection. If not some amount of chin pad ptosis will occur as the soft tissues have been expanded in front of the bone from the implant.The expanded soft tissues that aren’t picked up by the bone advancement risk contracting and creating vestibule and lower lip tightness. That type of chin effect its often associated with some degree of lower lip incompetence as well.
When performing a secondary chin augmentation with a sliding genioplasty let the bone make the needed horizontal, vertical or combined dimensional changes. Filling in the step off of the sliding genioplasty, if significant can bone done with an implant if a wider chin shape is desired. But the tissue tightness induced by the prior surgeries indicates a soft tissue deficiency for which a soft tissue graft (dermal-fat graft) is always the chest choice. The interesting and very relevant question is will a dermal-fat graft survive sitting on top of a chin implant?
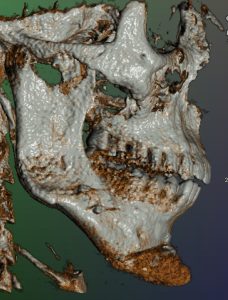
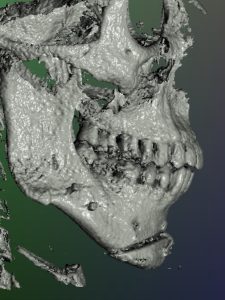 Case Study: This young male initially had a large chin implant through an intraoral approach which ultimately turned out to be too big. (too wide) Another surgeon removed the chin implant and replaced it with a sliding genioplasty of the same horizontal projection. (allegedly) But the result was seen as being too small and a 3D CT scan showed that the sliding genioplasty was only done out to 4mms. He also developed soft tissue chin pad ptosis, tightness and lower lip sag.
Case Study: This young male initially had a large chin implant through an intraoral approach which ultimately turned out to be too big. (too wide) Another surgeon removed the chin implant and replaced it with a sliding genioplasty of the same horizontal projection. (allegedly) But the result was seen as being too small and a 3D CT scan showed that the sliding genioplasty was only done out to 4mms. He also developed soft tissue chin pad ptosis, tightness and lower lip sag.


 I subsequently treated him with a triple genioplasty technique with a more substantial sliding genioplasty (with vertical shortening), an overlay chin implant and a dermal-fat graft on top of the implant to add soft tissue thickness and relieve the tightness.
I subsequently treated him with a triple genioplasty technique with a more substantial sliding genioplasty (with vertical shortening), an overlay chin implant and a dermal-fat graft on top of the implant to add soft tissue thickness and relieve the tightness.

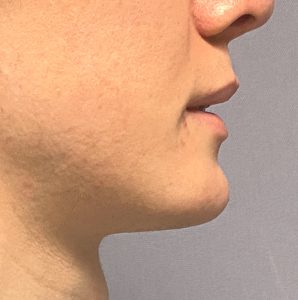
He had substantial improvement and when seen six months later he desired a small reduction in the projection of his chin and any further improvement possible in lifting his chin pad up. (which already had good improvement)

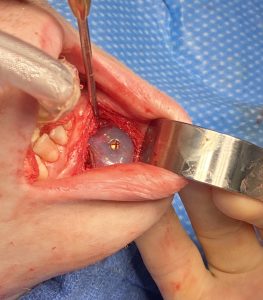
 Under general anesthesia and through his existing intraoral incision in dissecting down to the chin implant the dermal-fat graft was seen which was evidence it had some significant survival.
Under general anesthesia and through his existing intraoral incision in dissecting down to the chin implant the dermal-fat graft was seen which was evidence it had some significant survival.

 The silicone chin implant was removed. It was replaced by a modified/reduced ePTFE=coated silicone chin implant for the reduced horizontal projection. A suture was passed down through the implant on one side, grabbing the lower end of the soft tissue chin pad and then passed back through the implant on the other side. The implant was pushed down into the pocket and the suture pulled tight against the implant from above. It was tied to the residual stump of the mentalis muscle and the dermis of the fat graft to create an uplift off the chin pad to the implant. After the placement of antibiotic powder the incision was closed in multiple layers with resorbable sutures.
The silicone chin implant was removed. It was replaced by a modified/reduced ePTFE=coated silicone chin implant for the reduced horizontal projection. A suture was passed down through the implant on one side, grabbing the lower end of the soft tissue chin pad and then passed back through the implant on the other side. The implant was pushed down into the pocket and the suture pulled tight against the implant from above. It was tied to the residual stump of the mentalis muscle and the dermis of the fat graft to create an uplift off the chin pad to the implant. After the placement of antibiotic powder the incision was closed in multiple layers with resorbable sutures.
Getting complete correction in chin pad sagging (ptosis) is a challenge and is rarely achieved. Very good corrections can occur and some are almost complete. One of the keys to good corrections is having a ledge for the uplifted soft tissue pad to hang unto (in this case a combined bone-implant ledge) and a secure method to fix the chin pad onto this ledge. In this case a unique suture method through the implant was used due to its primary silicone composition with the added benefit of an ePTFE coating to further encourage soft tissue adherence.
Key Points:
1) A dermal-fat graft placed over a previous implant from a triple genioplasty showed good survival over an implant.
2) Tertiary chin pad re-suspension can be done with horizontal mattress sutures placed through the implant.
3) The threaded implant with ePTFE material provides a good surface for tissue ingrowth and soft tissue pad adherence.
Dr. Barry Eppley
World-Renowned Plastic Surgeon