

Background: Chin implants are the most common form of aesthetic facial augmentation and have been used ion various forms for more than a half century. Despite their frequent use by a wide variety of surgeons there remain numerous misconceptions about their placement, implant selection and the biologic response to them. This particular case study helps provide some clarity on a number of chin implant issues.
Case Study: This young male desired to undergo implant augmentation to improve his weak chin and jawline. He wanted improved chin projection as as well as a more square chin shape. He felt a sliding genioplasty was too invasive and preferred an intraoral approach. He went out of the US for the surgery.
 The procedure was done intraorally with a 10mm chin implant. His interpretation of the result was that it made little difference, despite the large implant, did not improve the shape of his chin and felt very high on the chin bone.
The procedure was done intraorally with a 10mm chin implant. His interpretation of the result was that it made little difference, despite the large implant, did not improve the shape of his chin and felt very high on the chin bone.
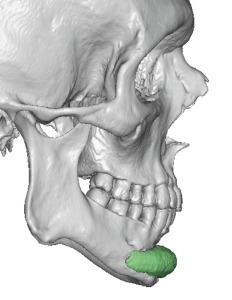 A 3D CT showed that a large round implant had been used and it was sitting up into the concave portion of the chin bone underneath the labiomental fold.
A 3D CT showed that a large round implant had been used and it was sitting up into the concave portion of the chin bone underneath the labiomental fold.
The concept of scarless intraoral chin implant placement has its obvious appeal but all too often the implant position ends up high. This does not allow the implant to exert its full horizontal projection effect and can even obliterate the labiomental fold. Some patients may even feel a full in the depth of the intraoral vestibule inside the lower lip. Making sure the dissection is done around the curve of the bottom part of the chin bone and using screw fixation to hold it down into place will avoid these problems.
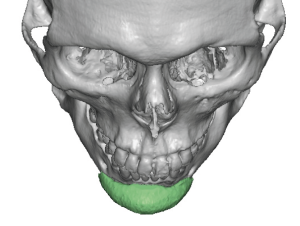 The 3D CT scan also shows clearly the round shape of the implant as seen from the top view.
The 3D CT scan also shows clearly the round shape of the implant as seen from the top view.
While it is obvious that an anatomic rounded shape implant can not make the chin more square why was it then used based on the patient’s request? In the short chin a large round implant is only going to make it more round or pointy as the projection is increased.
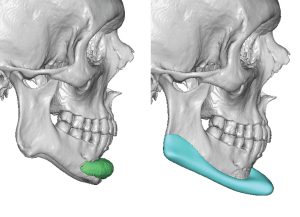
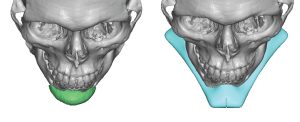 The patient desired to have a custom jawline implant replacement tis improve his chin issues as well as augment the entire jawline. Using his 3D CT scan a jawline implant was designed that added more chin projection, made the chin square as well as augmented the entire jaw behind it.
The patient desired to have a custom jawline implant replacement tis improve his chin issues as well as augment the entire jawline. Using his 3D CT scan a jawline implant was designed that added more chin projection, made the chin square as well as augmented the entire jaw behind it.
Some male patients with inadequate chin implant results will graduate to a custom implant to more assuredly improve the existing implant problems. That often encourages a more complete lower third of the face augmentation rather than just the chin. In making such an implant design the chin can definitively be made more square.

 The chin implant removal was done through a submental incision where initially then chin implant was not readily found. A ledge of bone was found higher up on the chin and it became apparent this was complete bone overgrowth around the chin implant. The bone was chipped away revealing the implant.
The chin implant removal was done through a submental incision where initially then chin implant was not readily found. A ledge of bone was found higher up on the chin and it became apparent this was complete bone overgrowth around the chin implant. The bone was chipped away revealing the implant.

 Once the implant was removed the numbers that were printed on the back side of the implant could be seen on the bone indicating some settling of the implant into the cortical surface.
Once the implant was removed the numbers that were printed on the back side of the implant could be seen on the bone indicating some settling of the implant into the cortical surface.
 The implant had holes on its wings and bone ingrowth could be seen that has occurred through it once the implant was removed.
The implant had holes on its wings and bone ingrowth could be seen that has occurred through it once the implant was removed.
The concept of bone erosion, most commonly associated with chin implants due to their frequency of use, can be seen there as a biologic misinterpretation. Erosion implies an inflammatory reaction to an irritant that melts bone, creates reactive granulation tissue and does not stop until the source is removed. This is clearest not what is being seen here. This is a clear example of passive bone remodeling to the pressure of an implant placed between the hard bone surface and the tight overlying soft tissues. This is a passive process which is seen by crisp bone edges, no signs of any inflammatory changes and the reparative response of bone over- and ingrowth. Essentially the body has accepted the implant but must adapt to its presence into a tissue site which had not been developed to contain it. The higher the implant is on the chin bone the greater the imprinting and reparative bony response that is seen nearer the concave surface of the upper chin bone.
 The inadequacies of a prior chin implant provide valuable information when one elects to move onward with a more complete jaw augmentation implant.
The inadequacies of a prior chin implant provide valuable information when one elects to move onward with a more complete jaw augmentation implant.
Key Points:
1) Highly positioned chin implants exhibit the highest occurrence of bone imprinting and bony ingrowth. (confirming the biologic misinterpretation of bone erosion)
2) Anatomic round chin implants create a pointy chin not a square one.
3) A custom jawline implant is a frequent replacement for indesired chin implant results.
Dr. Barry Eppley
World-Renowned Plastic Surgeon