


Background: Chin augmentation by either an implant or a sliding genioplasty can be a very effective lower facial enhancement for many patients. But given the length and surface area of the jawline it is important to remember that it occupies only about 20% of the total surface area of the bony lower face. Thus it chin augmentation alone can be eventually perceived by some as having an incomplete lower facial effect, prompting the desire for a total jawline implant.
Graduating from a chin to a complete jawline implant carries with it some certain and uncertain considerations. The known effect of the existing chin implant allows the front end of the jawline implant to be designed with a fair amount of certainty. What lies within guides how to make definite implant shape and size improvements. The larger posterior/jaw angle implant design, however, has no indwelling implant to help guide how it should be made. This requires preoperative computer imaging and an understanding of jaw angle implant design principles. (for which there are no written guidelines as it must rely on surgeon experience)
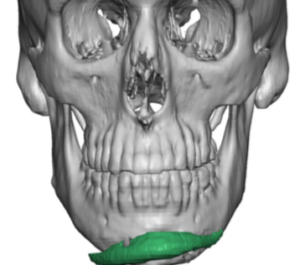
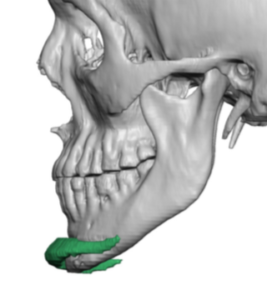 Case Study: This male had a prior chin implant from which he never was really happy with its aesthetic effect. Besides getting an improved chin shape (stronger and more square) he wanted a complete and profound jawline effect. His 3D CT scan show a chin implant with tilt asymmetry as the right wing was below the bone and the left wing positioned high up on the bone.
Case Study: This male had a prior chin implant from which he never was really happy with its aesthetic effect. Besides getting an improved chin shape (stronger and more square) he wanted a complete and profound jawline effect. His 3D CT scan show a chin implant with tilt asymmetry as the right wing was below the bone and the left wing positioned high up on the bone.
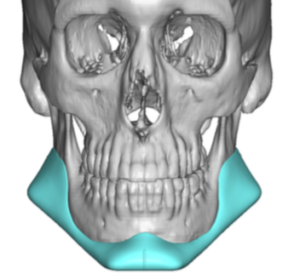
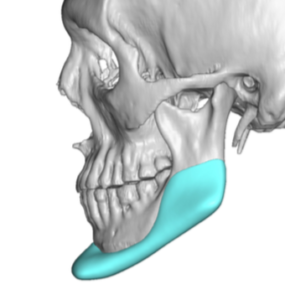
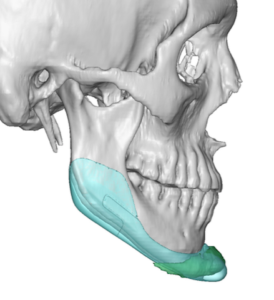
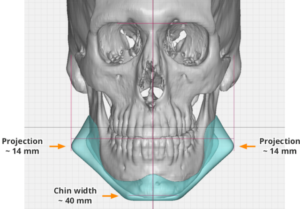 A custom jawline implant was designed creating a more square chin shape with increased horizontal projection. The jaw angle design included significant vertical lengthening and width. The connection between the chin and jaw angles was a linear one. Total implant volume was 26ccs. (which is definitely on the big side of jawline implants)
A custom jawline implant was designed creating a more square chin shape with increased horizontal projection. The jaw angle design included significant vertical lengthening and width. The connection between the chin and jaw angles was a linear one. Total implant volume was 26ccs. (which is definitely on the big side of jawline implants)
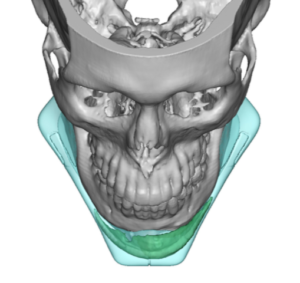
 Comparative overlay assessment of the new jawline implant design to that of the chin implant shows the differences in shape and bone coverage. (known area of design)
Comparative overlay assessment of the new jawline implant design to that of the chin implant shows the differences in shape and bone coverage. (known area of design)


 Under general anesthesia a submental incision was initially used to remove the indwelling chin implant and reduce the bony overgrowth around it. The complete subperiosteal pocket was created using two additional intraoral incisions for a three incisional technique. (anterior external submental and bilateral posterior intraoral vestibular incisions) Once the implant was inserted through the submental incision and in position the chin portion was secured with a superior screw with a 1mm reduction of its anterior projection by scalpel shaving. The jaw angles were positioned using the intraoral incisions with percutaneous placement of double screws through each implant angle to the bone.
Under general anesthesia a submental incision was initially used to remove the indwelling chin implant and reduce the bony overgrowth around it. The complete subperiosteal pocket was created using two additional intraoral incisions for a three incisional technique. (anterior external submental and bilateral posterior intraoral vestibular incisions) Once the implant was inserted through the submental incision and in position the chin portion was secured with a superior screw with a 1mm reduction of its anterior projection by scalpel shaving. The jaw angles were positioned using the intraoral incisions with percutaneous placement of double screws through each implant angle to the bone.
The stronger one goes with an initial chin augmentation the more likely the rest of the jawline will eventually look deficient by comparison. In this case with an initial 11mm chin implant (biggest that is made in standard sizes) his high jaw angles eventually became disproportionate in appearance.
 This illustrates that one of the key concepts in custom facial implants over standard facial implants is the amount of bone surface area coverage. In essence custom facial implants are designed to create an overall enlargement of larger bone surfaces like they are a natural growth/development of the entire bone. (looks like they belong there) By contrast standard facial implants are ‘spot’ implants enlarging smaller sections of the bone which work well when modest augmentations are done but can look ‘out of place’ when the such spot augmentations become too large.
This illustrates that one of the key concepts in custom facial implants over standard facial implants is the amount of bone surface area coverage. In essence custom facial implants are designed to create an overall enlargement of larger bone surfaces like they are a natural growth/development of the entire bone. (looks like they belong there) By contrast standard facial implants are ‘spot’ implants enlarging smaller sections of the bone which work well when modest augmentations are done but can look ‘out of place’ when the such spot augmentations become too large.
Case Highlights:
1) Chin augmentation can eventually be perceived as a subtotal jawline effect, prompting the desire for a more complete jawline augmentation result.
2) The chin can be the most straightforward part of a jawline implant design when an indwelling chin implant exists.
3) Larger jawline implant designs are when each of the corners exceeds double digits in millimeter augmentations and/or the implant volume is well over 20ccs.
Dr. Barry Eppley
Indianapolis, Indiana