


Background: Shoulder dysphoria is a perception that the width of one’s shoulders is disproportionately wide compared to other body features and dimensions. It is particularly associated with the transfemale population where the width of the shoulders can be a particularly sensitive issue in how the body is seen. There are anthropometric measurements for shoulder width in which that perception can be confirmed. Generally when the bideltoid distance is greater than 45 mms it is regarded as being outside the norm for females. In the hundreds of transfemale patients that I have treated every single one of them has been north of 45cms bideltoid measurement with a few as high as 52 cms.
But shoulder dysphoria is not an exclusive entity to transfemales alone. Cis-females can have it also although its occurrence is far less. There are many cis-females with broad/wide shoulders in which it is not a concern at all. In cis-females that have shoulder dysphoria they often have a predicate history of being teased about their shoulders when they were young.Having been told that one has ‘linebacker’ shoulders is a classic example that I hear. There are also issues of the fitting of clothes where the width of the the shoulders causes fit issues below it…and clothes that fit at the waistline are too tight at the shoulder.
In shoulder reduction surgery there is no difference between trans or cis-females in how the procedure is performed. The goal is still maximal clavicle bone removal based on the length of the bone and the plate that is applied.
Case Study: This female had long been bothered by the width of her shoulders having been teased about it when she was young. Her bideltoid distance was 48cms. She has broad shoulders with thick soft tissues with no clavicle show.

 Under general anesthesia and in the supine position a 2.5cm length of clavicle bone was removed from each side through small supraclavicular skin incisions. Double 2.0mm plates and screw fixation was applied after the blunt ends of the cut bone were put together. The thickness of the soft tissue over the clavicle was an 1 1/2 inch thick, making working through the small incision difficult.
Under general anesthesia and in the supine position a 2.5cm length of clavicle bone was removed from each side through small supraclavicular skin incisions. Double 2.0mm plates and screw fixation was applied after the blunt ends of the cut bone were put together. The thickness of the soft tissue over the clavicle was an 1 1/2 inch thick, making working through the small incision difficult.



 She went on to heal uneventfully and was not seen back for two years at which time she desired her hardware to be removed. Her supraclavicular scars were very acceptable with minimal show.There was no hardware show as would be expected with thick overlying soft tissues. She was happy with her result and felt it made a big difference in her appearance.
She went on to heal uneventfully and was not seen back for two years at which time she desired her hardware to be removed. Her supraclavicular scars were very acceptable with minimal show.There was no hardware show as would be expected with thick overlying soft tissues. She was happy with her result and felt it made a big difference in her appearance.

 Her supraclavicular incisions healed well with only slight scarring.
Her supraclavicular incisions healed well with only slight scarring.
 Her reason for hardware removal was that the right arm when reaching back felt like it got ‘caught’ or snagged. Her hardware was removed uneventfully. The left clavicle was fully healed with no evidence ofnthe original apposition of the union of the two bone ends. On the right side there was some visibility of the osteotomy line but with no bone instability.
Her reason for hardware removal was that the right arm when reaching back felt like it got ‘caught’ or snagged. Her hardware was removed uneventfully. The left clavicle was fully healed with no evidence ofnthe original apposition of the union of the two bone ends. On the right side there was some visibility of the osteotomy line but with no bone instability.
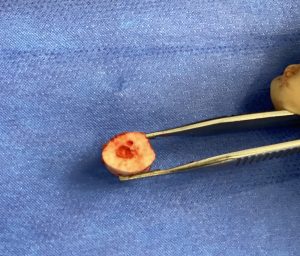 The bone of the clavicle has two layers, an inner marrow core surrounded by a circumfererntial wrap of dense cortical bone. The ratio between these two is a bit different in each patient, some having a greater marrow core while in others it is smaller. But regardless of this ratio in clavicle bone fixation it is important that the screws obtain purchase of the threads on both sides of the bone. (bicortical screw purchase) This is more important than the thickness of the plate used as fixation occurs by screw pullout and not by plate bending or breaking.
The bone of the clavicle has two layers, an inner marrow core surrounded by a circumfererntial wrap of dense cortical bone. The ratio between these two is a bit different in each patient, some having a greater marrow core while in others it is smaller. But regardless of this ratio in clavicle bone fixation it is important that the screws obtain purchase of the threads on both sides of the bone. (bicortical screw purchase) This is more important than the thickness of the plate used as fixation occurs by screw pullout and not by plate bending or breaking.
Key Points:
1) Shoulder dysphoria can also affect cis-females and not just transgender patients.
2) Lack of clavicle show indicates either a thick soft tissue cover or a thin clavicle bone.
3) Double plate fixation is indicated particularly in broader shoulders with thick soft tissues.
Dr. Barry Eppley
World-Renowned Plastic Surgeon