

Background: Shoulder narrowing surgery works by shortening the length of the clavicle bone. While this concept is straightforward as well as the execution of the surgery to do it, the clavicle is not a straight segment of bone. Its lazy-S shape combined with its various cross-secttional diameters throughout its length makes certain aspects of the surgery a little less than straightforward.
The shape of the clavicle is uniquely different and more highly variable than most other long bones. It has significant gender differences with the male clavicle being longer and thicker than in females. The left clavicle is almost always longer and a bit thinner than the right. The thickness of the clavicle bone also varies with the thickest cross-sectional area being age its sternal end, averaging around 20 to 22mms,. On the opposite acromial end the thickness drops significantly down to around 14 to 15mms.
In essence the cross-sectional thickness of the bone changes/drops along its length.. This explains a common observation that is seen in most clavicle reduction patients. When the two ends of the bone are put back together their cross-sectional diameters do not match. The acromial or distal end is smaller than the sternal or medial end. While at the superior surface I put the two ends together so there is a smooth continuous surface. But if you look on the underside the discrepancy between the thickness of the two bone ends is apparent.
Case Study: This female desired shoulder reduction with a bideltoid distance of 47cms and a clavicle length of 16cms

 Under general anesthesia and through 3.5cms supraclavicualr fossa incisions, 2.5cms of bone was removed from the mid-shaft portion of the clavicles. The distal end of the clavicle was moved to an end-to-end abutment with the medial end and secured with double plate fixation. At the superior and anterior views across the fixation line there was perfect alignment.
Under general anesthesia and through 3.5cms supraclavicualr fossa incisions, 2.5cms of bone was removed from the mid-shaft portion of the clavicles. The distal end of the clavicle was moved to an end-to-end abutment with the medial end and secured with double plate fixation. At the superior and anterior views across the fixation line there was perfect alignment.

 The intraoperative change in shoulder width was immediately apparent.
The intraoperative change in shoulder width was immediately apparent.
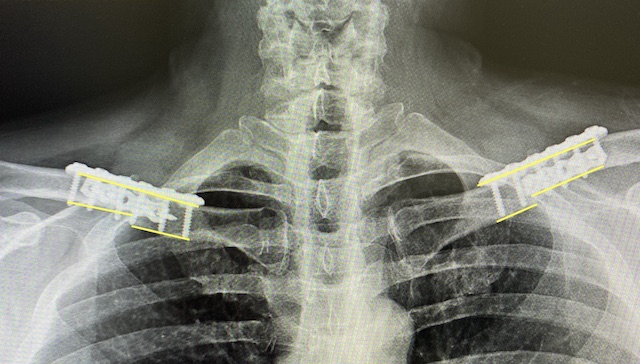
 Postoperative x-rays showed good segment alignment and stable plate fixation with good bicortical screw placement. A visible change in the thickness of the bone could be seen on the underside with a 1/3 reduction in the size of the distal segment to the proximal segment.
Postoperative x-rays showed good segment alignment and stable plate fixation with good bicortical screw placement. A visible change in the thickness of the bone could be seen on the underside with a 1/3 reduction in the size of the distal segment to the proximal segment.
I continue to find ways that clavicle reduction osteotomies are not similar to clavicle fracture repair. The common difference in the size of the two bone ends that are put back together is another example of their differences. Clavicle fracture repair is about re-establishing clavicle length and thicknesses. Clavicle reduction osteotomies are about decreasing bone length with the unintentional but inevitable discrepancy is cross-sectional bone thicknesses across the osteotomy. This appears to have no relevance to primaryhealing but may have some significance if the hardware is removed in the early healing period of that surgery.
Case Highlights:
1) The fundamental concept of shoulder narrowing surgery is to remove a segment of the mid-shaft portion of the clavicle.
2) Despite removing a relative small section of the bone, compared to its overall length, when the two segments are brought together they are discrepant in size.
3) While the dissimilar cross-sectional diameters of the reunited clavicle bone has never posed an obvious postoperative issue it may have some relevance in the early healing if the hardware is ever removed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon