


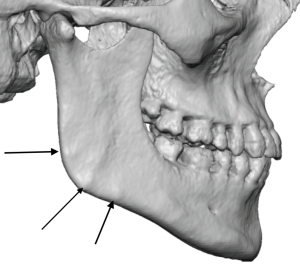
 Background: The masseter muscle is one of major lower jaw soft tissue structure that not only contributes to its movement but adds width to the face as well. It has a broad origin along the zygomatic arch and narrows down into a triangular shape at its insertion point over the bony jaw angle. It attaches to the jaw angle through numerous ligaments which are quote stout and very pronounced in many men. Such ligamentous attachments can be clearly identified in 3D CT scans as bony bumps along the inferior border of the jaw angles. They are more pronounced in men than women with many women having no evidence of them at all.
Background: The masseter muscle is one of major lower jaw soft tissue structure that not only contributes to its movement but adds width to the face as well. It has a broad origin along the zygomatic arch and narrows down into a triangular shape at its insertion point over the bony jaw angle. It attaches to the jaw angle through numerous ligaments which are quote stout and very pronounced in many men. Such ligamentous attachments can be clearly identified in 3D CT scans as bony bumps along the inferior border of the jaw angles. They are more pronounced in men than women with many women having no evidence of them at all.
In placing jaw angle implants the massteric muscle poses challenges. Through an intraoral approach it must be elevated off of the bone to create the implant pocket. How much to elevate the along the inferior border is the question that must bgve determined for each patient and jaw angle implant style used. When a widening jaw angle implant is used the ligamentous attachments may only need to be partially for incompletely released. But when the implants is needed to create any amount of vertical lengthening the ligamentous attachments must be fully released.
In fully releasing the massteric ligamentous attachments there is always the risk of developing postoperative masseteric muscle dehiscence. (retraction of the muscle upwards towards its origin) While this does not cause any functional issues it does create a soft tissue deficiency over the jaw angle resulting in implant show. While there are other forms of jaw angle surgery where the ligaments are released, and masseteric muscle dehiscence is not seen, it is the placement of an implant between the bone and the muscle that allows its retraction to occur. Masseteric muscle dehiscence does not occur with ligamentous release for implant placement if the periosteal attachments that wrap around the inferior border are preserved. But these attachments are thin and easily disrupted. The amount of vertical jaw angle lengthening also plays a factor in the risk of masseteric muscle dehiscence occurring.
While the anatomic approach to the treatment of masseteric muscle dehiscence is muscle repositioning this secondary surgery has a low success rate and results in an external scar. Camouflage treatments are injectable approaches with fillers and fat which can be effective in more minor or modest jaw angle contour deformities. Another effective option in more significant muscle retraction deformities is a soft tissue implant approach.

 Case Study: This male had prior jaw angle implant surgery with significant bilateral masseteric muscle dehiscence. Given the magnitude of the muscle retraction and the years it had been present a camouflage implant approach was taken.
Case Study: This male had prior jaw angle implant surgery with significant bilateral masseteric muscle dehiscence. Given the magnitude of the muscle retraction and the years it had been present a camouflage implant approach was taken.

 Ultrasoft solid silicone jaw angle implants were made based on the triangular measurements of the exposed jaw angle implant and muscle retraction. The implant had to have enough surface area coverage that the hypotenuse side of the implant extended up over the retracted muscle edge. The implant width at the lower jaw angle area was 4mms.
Ultrasoft solid silicone jaw angle implants were made based on the triangular measurements of the exposed jaw angle implant and muscle retraction. The implant had to have enough surface area coverage that the hypotenuse side of the implant extended up over the retracted muscle edge. The implant width at the lower jaw angle area was 4mms.

 Through a small direct incision over the jaw angles a subcutaneous pocket was created preserving the capsule over the underlying implant. An adequate but not over dissected implant pocket is needed through onto which the implant is placed. To improve soft tissue fixation and add extra width a 2mm thick ePTFE patch is placed under the angle area of the implant and sutured to it. Then both implants are sutured to the soft tissue underneath it.
Through a small direct incision over the jaw angles a subcutaneous pocket was created preserving the capsule over the underlying implant. An adequate but not over dissected implant pocket is needed through onto which the implant is placed. To improve soft tissue fixation and add extra width a 2mm thick ePTFE patch is placed under the angle area of the implant and sutured to it. Then both implants are sutured to the soft tissue underneath it.

 Two layer skin closure was done with resorbable sutures. No drains were used.
Two layer skin closure was done with resorbable sutures. No drains were used.
Masseteric muscle dehiscence, while not a functional problem, is a pesky aesthetic one. It can mar the best jaw angle implant results when it occurs. Fortunately it is not common with good surgical technique but the risk is always present. in established muscle dehiscence that defies resolution with injection techniques a soft tissue implant can be an effective option. Most don’t think of placing implants in the soft tissues although there is a precedent history in the lips with both ePTFE and solid silicone. There is no reason that such implants can not be placed in other soft tissue sites in the face. Getting good placement in the soft tissues of the jaw angles can only be done by a more direct approach using either an angle skin incision or one placed around the base of the earlobe. The key to a successful soft tissue jaw angle contour augmentation is an ultrasoft silicone material that has feather edges with the exception of need width at the angle area. Such feathering is important to avoid potential visible implant edging when the implant site is fully healed.
Case Highlights:
1) Masseteric muscle dehiscence is a not uncommon sequelae from aesthetic jaw angle implant surgery creating a soft tissue contour deformity.
2) One effective treatment approach is the placement of a soft tissue jaw angle implant through a transcutaneous approach.
3) The combination of an ePTFE patch on the inner aspect of the soft tissue jaw angle implant helps ensure soft tissue fixation as well as adds extra width.
Dr. Barry Eppley
World-Renowned Plastic Surgeon