


Background: The chin is a unique facial structure being a solitary projection that is enveloped by a tight soft tissue chin pad. The chin pad is composed of periosteum, muscle, fat and skin that is adherent around the bone. Like all structural manipulations anywhere on the face how the soft tissue drapes over it does impact the aesthetic outcome. In the chin this soft tissue adaptation is never a problem in augmentation surgery (bony genioplasty and implants) because the soft tissue is expanded and postoperative laxity of it is not a concern.
In chin reductions, however, the adaptation of the soft tissue chin pad to a reduced structural support is another matter. This is most manifest in intraoral bony chin reductions by shaving/burring in which the overlying adherent soft tissues have been elevated off of the bone. With less bony support a relative soft tissue excess results which any surgeons assume will merely contract back down and the bone-soft tissue ratio restored. But this is a misconception and some soft tissue laxity will always occur. Whether this newly created soft tissue chin pad excess/laxity is a concern depends on its significance as well as the patient’s perception of it.
Should soft tissue chin pad excess/laxity occur and is a perceived concern the question becomes how to best manage it. It is appealing to try and resuspend the soft tissues intraorally but soft tissue excesses are not usually resolved by lifting. Like soft tissue excesses anywhere on the body excision is the definitive treatment.

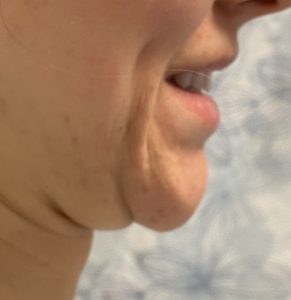 Case Study: This female had previously undergone an intraoral chin reduction contouring procedure in which the chin projection was reduced by a sagittal saw after degloving of the soft tissues. This eventually resulted in the sequelae of a double roll chin pad deformity (chin pad ptosis with a submental roll) which was most evident when smiling. The plan was to reduce enough of the soft tissue chin pad to reduce its projection a little at rest and reduce the rolls when smiling.
Case Study: This female had previously undergone an intraoral chin reduction contouring procedure in which the chin projection was reduced by a sagittal saw after degloving of the soft tissues. This eventually resulted in the sequelae of a double roll chin pad deformity (chin pad ptosis with a submental roll) which was most evident when smiling. The plan was to reduce enough of the soft tissue chin pad to reduce its projection a little at rest and reduce the rolls when smiling.

 Under general anesthesia and using a horizontal submental skin crease as the posterior incision, an elliptical excision of redundant soft tissue chin pad was marked out for excision. Once the skin, fat and muscle of the marked area was excised, the difference in the levels of the chin and submental neck tissues was apparent.
Under general anesthesia and using a horizontal submental skin crease as the posterior incision, an elliptical excision of redundant soft tissue chin pad was marked out for excision. Once the skin, fat and muscle of the marked area was excised, the difference in the levels of the chin and submental neck tissues was apparent.


 A direct excision of the submental fat on the posterior side of the incision was done to level out the two sides. The two sides of the excision were brought together and were much more level. To complete the leveling between the chin pad and the submental neck, small cannula liposuction was done of the submental region. The final skin closure with resorbable sutures followed.
A direct excision of the submental fat on the posterior side of the incision was done to level out the two sides. The two sides of the excision were brought together and were much more level. To complete the leveling between the chin pad and the submental neck, small cannula liposuction was done of the submental region. The final skin closure with resorbable sutures followed.


 She was seen five years later where the long term outcome of the procedure and the scar could be fully appreciated. The submental scar was virtually invisible and only a minor soft tissue chin pad roll remained with completion elimination of the submental roll when smiling.
She was seen five years later where the long term outcome of the procedure and the scar could be fully appreciated. The submental scar was virtually invisible and only a minor soft tissue chin pad roll remained with completion elimination of the submental roll when smiling.

 She was seen back after five years as she wanted a touch up of her original procedure with just a little more soft tissue chin pad removed. This was done using her original scar with anterior excision of more soft tissue. I would expect the submental scar to end up as good as it did the first time.
She was seen back after five years as she wanted a touch up of her original procedure with just a little more soft tissue chin pad removed. This was done using her original scar with anterior excision of more soft tissue. I would expect the submental scar to end up as good as it did the first time.
Case Highlights:
1) intraoral chin and jaw bony reduction require soft tissue stripping from the bone and its results partially depend on soft tissue contraction…which may not reliably occur particularly of the soft tissue chin pad.
2) Excessive soft tissue chin pad may develop after intraoral bony chin reduction which is most manifest when smiling.
3) Tightening of the lax soft tissue chin pad can only reliably be done from an external submental approach which is ideally placed in a skin crease if it exists.
Dr. Barry Eppley
World Renowned Plastic Surgeon