

Background: Body contouring in the transgender male to female patient is fundamentally about creating curves which is associated with a more feminine appearance. There are a variety of procedures to do so including breast augmentation, waistline reduction and hip/buttock augmentation. Not every patient needs or wants all three areas treated although the best results comes from doing so. Breast augmentation is the most straightforward in which implants are unequivocally the most successful in doing so. Hip and buttock augmentation can be done with wither fat or implants depending upon how much one has to harvest. Waistline reduction can be done by traditional liposuction and in some cases a tummy tuck. More resistant waistlines require lower ribcage modification through rib removals.
Depending upon he body type (thin vs thicker) some of the body contouring procedures will be more effective than others. Thinner patients often require less of them while thicker framed bodies requires a maximum procedure approach. The key decision is around the waistline. While buttock augmentation has its benefits hip augmentation produces more of a visible change in frontal and back views. While hip augmentation can be done by both implants and fat, thicker framed bodies are better served by taking as much fat around the mid-body as possible and using it for the hip augmentation. Fat injections are not known for being very reliable in the hip area but it is always worth the initial effort as hip implants, which have a higher risk of complications, can always be done later if needed.
Rib removal waistline narrowing is well known but it is most effective in thinner body frames where the lower ribcage makes a more visible and greater contribution to its width. Thus in thicker body types an equal emphasis needs to be done on soft tissue around the lower ribcage. This refers to both fat and muscle. Fat removal is obvious but often overlooked is the contribution of the very thick and wide latissimus dorsi muscle.
![]() Case Study: This now female patient had a larger thicker frame in addition to the undesired straight body profile. An autologous approach to body contouring was planned which included a ‘removal and redistribution’ approach.
Case Study: This now female patient had a larger thicker frame in addition to the undesired straight body profile. An autologous approach to body contouring was planned which included a ‘removal and redistribution’ approach.
![]()
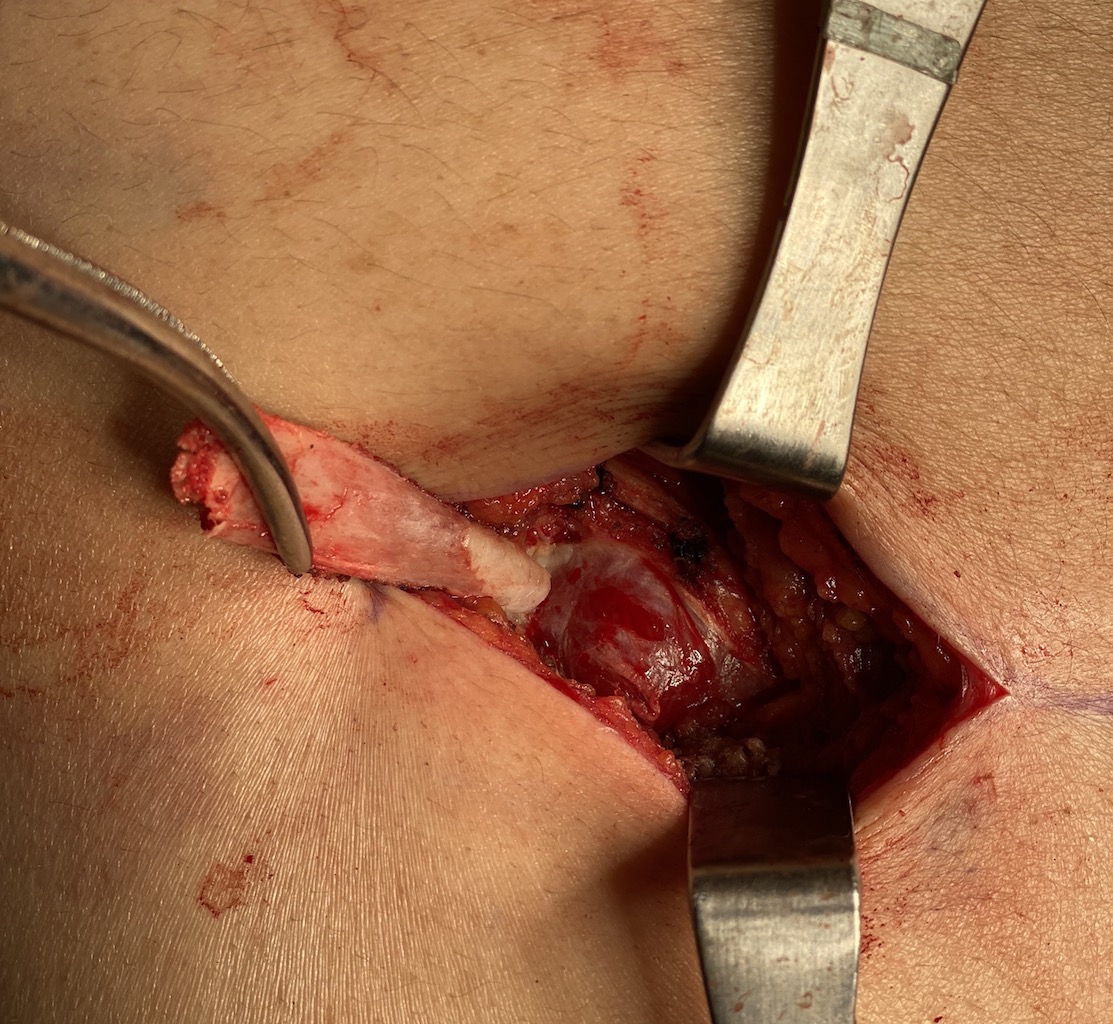
![]() Under general anesthesia and in the prone position the entire abdomen and anterior flanks was harvested of fat. Then in the prone position the posterior flanks and back were aspirated, creating a combined 1,575ccs of aspirate. After some concentration a total of 500cc of fat was injected into each hip region. Then through 5cm long back incisions, the outer half of ribs #11 and #12 were taken. (due to the exposure of pleura, ribs #10 were not removed) A large wedge of lastissimus dorsi muscle was harvested with the apex of the wedge along a circumferential line drawn around the umbilicus. Drains were placed from the rib removal areas back out through the liposuction entrance sites.
Under general anesthesia and in the prone position the entire abdomen and anterior flanks was harvested of fat. Then in the prone position the posterior flanks and back were aspirated, creating a combined 1,575ccs of aspirate. After some concentration a total of 500cc of fat was injected into each hip region. Then through 5cm long back incisions, the outer half of ribs #11 and #12 were taken. (due to the exposure of pleura, ribs #10 were not removed) A large wedge of lastissimus dorsi muscle was harvested with the apex of the wedge along a circumferential line drawn around the umbilicus. Drains were placed from the rib removal areas back out through the liposuction entrance sites.
To create some semblance of curves in a fuller straight-line body frame is challenging. Every tissue type and layer is thicker and more resistant to change. So doing as much as one can is the key beginning with aggressive liposuction and recycling the fat to the hips. Fat is maximally injected until the internal pressure of the injectate can only be held in by suturing the skin entrance sites. While taking as many lower ribs and their lengths as much as is safe is important the significance of removing the thick latissimus dorsi muscle that overlies them is just as important. The larger the wedge of muscle removal the better. There will be no functional loss of the action the muscle performs given is large surface area of coverage on the back.
Case Highlights:
1) Body contouring on the larger framed transgender male to female patient is challenging and requires a ‘maximum’ multilevel approach.
2) For the waistline you take rib #11 and #12 (#10 if possible) and, equally important, take a large wedge of the latissimus dorsi muscle.
3) Combine with hip augmentation by fat injections, harvesting as much fat as possible from the abdomen/flanks and back.
Dr. Barry Eppley
Indianapolis, Indiana