

Background: In breast augmentation surgery one of the primary goals is symmetry. While the implants may be symmetric in size and volume is not, however, a guarantee that the breasts will be perfectly symmetric afterwards. There are numerous anatomic components around, on top and underneath the breast implants that will play a significant role in how symmetric the two breast mounds will be.
Most of the time in breast augmentation the visible external soft tissue shape of the natural breast mounds is what can have the greatest impact on symmetry. But less commonly the shape of the underlying chest wall can play a major role as well. This is most significantly seen in congenital chest wall deformities such as pectus excavatum and Poland’s syndrome. In these well known chest wall disorder there is a ribcage deformity in which the natural curvature of the ribs is altered to a flatter or even a concave shape. This also can cause a midline deviation of the sternum to the affected side.
In such chest wall deformities this can be expected to affect the appearance of breast augmentation surgery as the base on which the implant sits is different between the two sides. In minor chest wall deformities having one breast implant bigger than the other may produce an acceptable amount of asymmetry. But in more significant chest wall asymmetries the platform on which the breast implant sits may need to be built up for the breast implant to work more effectively.
 Case Study: This middle aged female had a significant left pectus chest wall deformity that was diagnosed later in life for which she underwent reconstructive surgery. (Nuss procedure) Subsequent silicone breast implants were done with 550cc volume on the normal right side and 475cc volume on the left side. Not unexpectantly, significant breast mound asymmetry persisted/resulted.
Case Study: This middle aged female had a significant left pectus chest wall deformity that was diagnosed later in life for which she underwent reconstructive surgery. (Nuss procedure) Subsequent silicone breast implants were done with 550cc volume on the normal right side and 475cc volume on the left side. Not unexpectantly, significant breast mound asymmetry persisted/resulted.
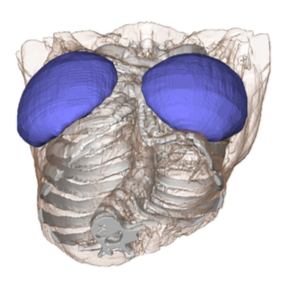 Using a 3D CT chest scan, the difference in the level of position of the breast implants could be seen.
Using a 3D CT chest scan, the difference in the level of position of the breast implants could be seen.
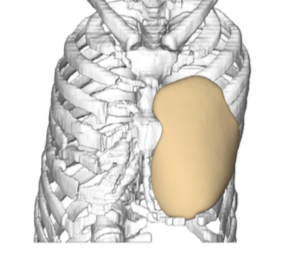
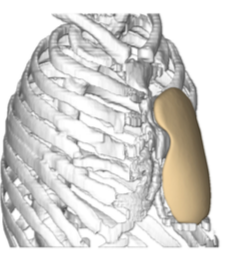 The 3D CT scan was used to create a left chest wall implant that elevated its depression to that of the opposite normal right side.
The 3D CT scan was used to create a left chest wall implant that elevated its depression to that of the opposite normal right side.
 Under general anesthesia her existing inframammary scar was opened and the indwelling breast implant removed. The surrounding and underlying breast implant capsule was preserved. The capsule was elevated off the chest wall superiorly up to the clavicle. This was important to keep the breast implant replacement and the custom chest wall implant into two separate pockets. Inferiorly all soft tissues were elevated off down to the subcostal rib margin.
Under general anesthesia her existing inframammary scar was opened and the indwelling breast implant removed. The surrounding and underlying breast implant capsule was preserved. The capsule was elevated off the chest wall superiorly up to the clavicle. This was important to keep the breast implant replacement and the custom chest wall implant into two separate pockets. Inferiorly all soft tissues were elevated off down to the subcostal rib margin.



 The custom chest wall implant was manufactured with ePTFE (Goretex) sheeting on its underside to help with postoperative soft tissue adhesion for fixation. Also multiple 6mm perfusion holes were placed throughout the implant to also assure soft tissue ingrowth. The implant was inserted placing it under the elected breast implant capsule.
The custom chest wall implant was manufactured with ePTFE (Goretex) sheeting on its underside to help with postoperative soft tissue adhesion for fixation. Also multiple 6mm perfusion holes were placed throughout the implant to also assure soft tissue ingrowth. The implant was inserted placing it under the elected breast implant capsule.

 The remaining breast implant capsule was expanded and a new 500cc silicone breast implant placed. The capsule was the closed inferiorly as well as the skin incision over it.
The remaining breast implant capsule was expanded and a new 500cc silicone breast implant placed. The capsule was the closed inferiorly as well as the skin incision over it.
When significant chest wall asymmetry exists due to a ribcage deformity a custom chest wall implant can be designed to even out the two sides of the chest. With improved chest wall symmetry breast implants of a more similar size can be used. The key to using a combination of chest wall and overlying breast implant is to keep two separate pockets as well as create means by which soft tissue fixation to the chest wall implant can occur. (as the material will not hold sutures)
Case Highlights:
1) Congenital chest wall deformities can affect the symmetry and size of breast augmentation surgery.
2) Uneven ‘flooring’ on which the breast implants sit can be hard to overcome merely changing breast implant sizes between the two sides when a major chest wall difference exists.
3) A custom chest wall implant evens out the two sides in certain congenital deformities that makes a breast augmentation result less asymmetric.
Dr. Barry Eppley
Indianapolis, Indiana