

Background: Of all aesthetic body implants they greatest unfulfilled need is for a hip implant. While historically the concept of hip augmentation was unknown today between cultural changes in aesthetic body shapes and the ubiquity of BBL surgery, to name the top two reasons, the desire for hip augmentation has become common. As an extension of BBL surgery the most common method of hip augmentation is fat injections…whose effectiveness is unpredictable due to the unknown postoperative fat survival by injection. But despite this well known ‘problem’ with fat injections it is still commonly done and may even be considered a primary approach in most patients because it has no postoperative complications and is the patients own tissues.
But when hip fat injections are inadequate the only other option is an implant. Despite this now contemporary need for a hip implant none exists as an off-the-shelf. As a result surgeons use either implants made for other body areas or have them custom made. But no matter what is used (and custom made implants are clearly superior to any other form of implant for the hips) they pose unique problems. Because of anatomic limitations the tissue pocket is not deep and the implant sits in a vertical orientation.This makes the hip implant prone to visible edging or even folding on its lower end.
What makes these potential hip implant issues even more relevant is in the thinner patient where the subcutaneous fat layer is thin. This is exactly the type of patient who is either not a good candidate for fat injections or where fat injections have proven inadequate. As a result large hip implants in thin patients should be avoided as the risk of complications is high. One good candidate for hip implants where the risk of complications is lower (I didn’t say zero) is in the hip dip indentation patient. The size of the hip implant needed is smaller as it sits between the iliac crest and the prominence of the greater trochanter of the femur.
Case Study: This female had prior body contouring procedures consisting of rib removal and taking the little fat she had and injecting it into her hip dips. To no surprise there was no fat survival and she now sought implants for a more effective and permanent solution.

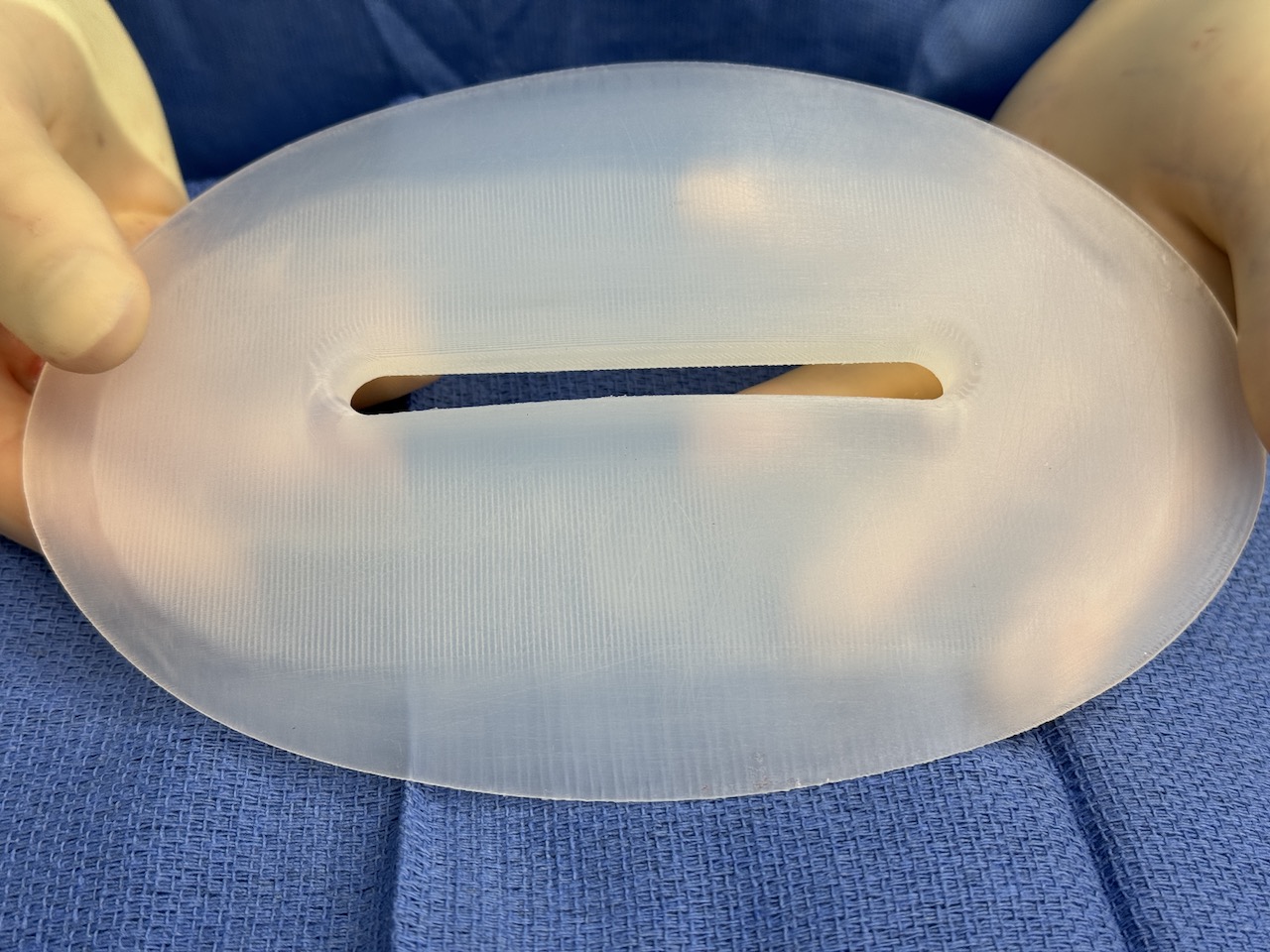
 Based on her hip dip measurements custom hip implants were designed to match their surface area with a maximum thickness of 1.5cms projection/thickness. To help with implant stability in there pocket a central channel was created down the middle of the implant (for tissue ingrowth) and ePTFE sheeting was applied to its undersurface. (for tissue adherence)
Based on her hip dip measurements custom hip implants were designed to match their surface area with a maximum thickness of 1.5cms projection/thickness. To help with implant stability in there pocket a central channel was created down the middle of the implant (for tissue ingrowth) and ePTFE sheeting was applied to its undersurface. (for tissue adherence)
 Under general anesthesia and alternating from the side to side intraoperative position the hip implants were placed through a small incision below the iliac crest on top of the deeper fascia. Closure of each side was done over a drain.
Under general anesthesia and alternating from the side to side intraoperative position the hip implants were placed through a small incision below the iliac crest on top of the deeper fascia. Closure of each side was done over a drain.

 When seen four months later her hip dips had been eliminated and she now had some hip shape which worked synergistically with her prior waistline narrowing procedure.
When seen four months later her hip dips had been eliminated and she now had some hip shape which worked synergistically with her prior waistline narrowing procedure.

 There was no visibility of the central channel on either implant despite the depth of and length of it. There was some inferior edging which was most evident on the left side.
There was no visibility of the central channel on either implant despite the depth of and length of it. There was some inferior edging which was most evident on the left side.

 Inferior hip implant visibility can occur for three reasons. First it is is a vertically oriented implant that sits on the side of the body. As the thinnest part of the implant is at the bottom and there is no adherence of the capsule to the implant, the weight of the implant can cause its bottom third to bend or sag creating a fold (implant buckle) which appears as a visible bulge externally. Secondly the pocket dissection at the time of implant placement may be .inadequate. This would most likely occur at the bottom of the implant,and when all the swelling goes down the edge of the implant will be bent as it can not lay flat. Third, the inferior edge of the dissection may have gotten away from the fascia and the inferior end of the dissection is up into the subcutaneous tissues. When the swelling goes down the edge of the implant will be visible.
Inferior hip implant visibility can occur for three reasons. First it is is a vertically oriented implant that sits on the side of the body. As the thinnest part of the implant is at the bottom and there is no adherence of the capsule to the implant, the weight of the implant can cause its bottom third to bend or sag creating a fold (implant buckle) which appears as a visible bulge externally. Secondly the pocket dissection at the time of implant placement may be .inadequate. This would most likely occur at the bottom of the implant,and when all the swelling goes down the edge of the implant will be bent as it can not lay flat. Third, the inferior edge of the dissection may have gotten away from the fascia and the inferior end of the dissection is up into the subcutaneous tissues. When the swelling goes down the edge of the implant will be visible.
The purpose of the two features on this hip implant design (central channel and ePTFE backing) is to support the implant so inferior edging by a bend does not occur. Thus the inferior edging in this case study could be due to a slightly inadequate pocket dissection or an inferior edge of the implant that is not laying completely flat on the fascia.
Key Points:
1) Thin tall females are prone to narrow hips evident by a hip dip concavity between the iliac crest and the greater trochanter of the femur.
2) The hip dip implant is limited surface area thin design with the goal to fill out the hip dip indentation placed on the deep fascia.
3) All hip implants are prone to inferior edging in thin patients due to the pocket location and their vertical orientation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon