

Background: Undereye hollows are a very common aesthetic concern. It occurs for a variety of anatomic reasons from fat atrophy/loss to skeletal deficiencies. The most common treatment is injectable fillers which can have good success but is not complication free. Irregularities and over/undercorrection are not uncommon post injection outcomes. But the one outcome issue that is uniformly shared with any injectable treatment is that it is not permanent and must be repeated.
Permanent undereye hollow treatments rely on some form of skeletal augmentation. Most commonly infraorbital implants of varying material compositions have been used. For small or selective area augmentations these type implants can produce satisfactory results. But the real cause of significant undereye hollows is skeletal-based and occurs along a long span of the orbital rim and extends out onto the malar eminence. It often is more of an orbito-zygomatic complex issue.
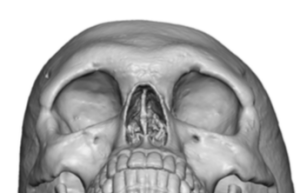
Often these more significant undereye hollow patients may have a negative orbital vector. They often have been through injectable filler treatments which have produced modest results and may take considerable volume with each injection treatment.A 3D CT scan will show the shape of the infraorbital rim and anterior alar area compared to the overlying brow bones and the rest of the facial bones.
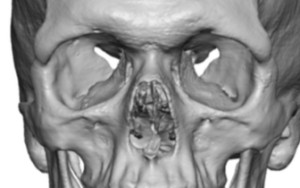
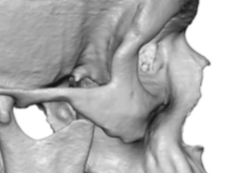
 Case Study: This male was bothered by undereye hollows which have been improved by injectable fillers but only modestly so. He desired a better and permanent treatment solution. A 3D CT scan showed an orbital rim deficiency that involved the lateral and inferior orbital rims. This was evident by the step off seen at the frontozygomatic suture line. (as opposed to a smooth transition which is normally seen)
Case Study: This male was bothered by undereye hollows which have been improved by injectable fillers but only modestly so. He desired a better and permanent treatment solution. A 3D CT scan showed an orbital rim deficiency that involved the lateral and inferior orbital rims. This was evident by the step off seen at the frontozygomatic suture line. (as opposed to a smooth transition which is normally seen)
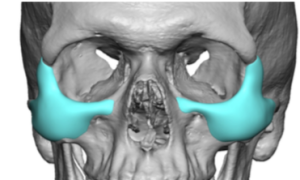
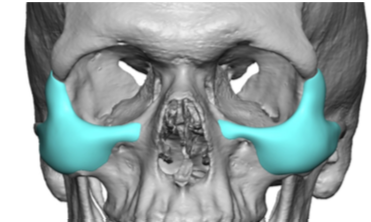
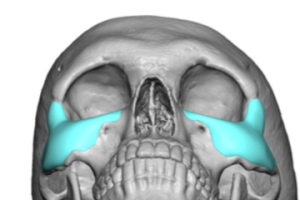 An undereye hollows custom implant was designed with augmented the deficient orbital rim with extended coverage out onto the anterior zygoma. This brought out the orbital rim area into closer alignment with that of the brow bones.
An undereye hollows custom implant was designed with augmented the deficient orbital rim with extended coverage out onto the anterior zygoma. This brought out the orbital rim area into closer alignment with that of the brow bones.



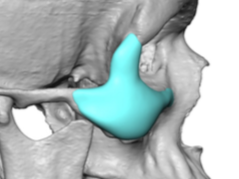
 Surgical placement of the custom infralateral orbital rim-malar implant is done through a lower eyelid incision. It is not necessary to have an incisional length across the whole lower eyelid…halfway or 3/4 length is the most that is needed. Once in good position i is secured with a single screw into the upper body of the zygoma.
Surgical placement of the custom infralateral orbital rim-malar implant is done through a lower eyelid incision. It is not necessary to have an incisional length across the whole lower eyelid…halfway or 3/4 length is the most that is needed. Once in good position i is secured with a single screw into the upper body of the zygoma.
For the motivated patient with a true skeletal basis for their undereye hollows who has injectable filler fatigue or has failed to get results from fat injections, the custom implant approach can provide permanent significant improvement. It will take about 3 weeks until one looks surgically inconspicuous. The risk of lower eyelid malformations is low when the use the lower lid incision is non-excisional in nature.
Case Highlights:
1) A zygomatic cheek deficiency can be anterior based and involve a backward tilt to the inferior and lateral orbital rims, creating a pseudo brow bone prominence and undereye hollow appearance.
2) The infralateral orbital rim deficiency can be seen in a 3D CT scan with a pronounced step off below the frontozygomatic suture line.
3) Custom infralateral orbital rim-malar implants can be inserted through a lower eyelid incision which is challenging due to its tripod shape.
Dr. Barry Eppley
Indianapolis, Indiana