

Background: Every bone on the face is capable of being underdeveloped and presents different aesthetic issues based on the area affected. The eye area is no different. One of the common periorbital skeletal deficiencies is that of the lower eyelid bone or infraorbital rim. Infraorbital rim recession may occur in isolation ut more commonly extends back to the anterior cheek bones as well given that they are connected and develop together.
When this orbital bone area is recessed the overlying soft tissues are correspondingly pulled back as well. This results in the appearance of lower eyelid bags due to the exposed infraorbital fat pads. (pseudofat herniation) The upper midface will appear flat and a side view will show that the corner of the eyeball is more forward than that of the infraorbital rim. (negative orbital vector) The front part of the cheekbone also has less projection although the more posterior arch component may have adequate with.
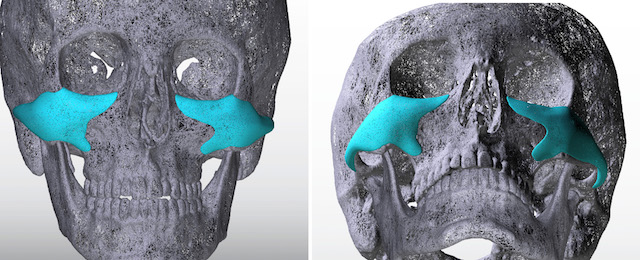
The aesthetic correction of infraorbital-malar hypoplasia has been done by various methods. But the ideal approach is to rebuild or augment the deficient bone in a connected and smooth fashion. This is best done using a custom implant approach based on the patient’s 3D CT scan. This allows for a preoperatively controlled shape and dimensions that will optionally fit the bone smoothly. When looking at such implant designs their size can be surprising given their surface area coverage.
Case Study: This young male presented with a desire to improve his undereye appearance. Even though he was young he had a flat sallow appearance to his lower eyes and had fat protrusions….all indicative of a developmental problem not an aging one. He also wanted a stronger cheekbone appearance.
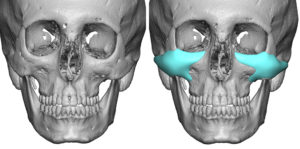
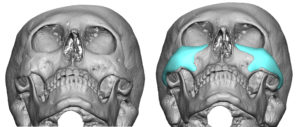 Using his 3D CT scan custom infraorbital-malar implants were designed to build up his infraorbital rims and provide a high cheek augmentation effect as well. The design provided a confluent augmentative effect from the side of the nose all the way back along the zygomatic arches. How much to build up the infraorbital rims is not an exact science but the horizontally and vertically deficiency infraorbital rims need a 3D change. This will also help the support to the lower eyelids as well.
Using his 3D CT scan custom infraorbital-malar implants were designed to build up his infraorbital rims and provide a high cheek augmentation effect as well. The design provided a confluent augmentative effect from the side of the nose all the way back along the zygomatic arches. How much to build up the infraorbital rims is not an exact science but the horizontally and vertically deficiency infraorbital rims need a 3D change. This will also help the support to the lower eyelids as well.
 Under general anesthesia a lower eyelid incision was made 1mm below the lash line and stopping just at a vertical line dropped down from the pupil. From this limited eyelid incision approach, subperiosteal dissection as done over the entire footprint of the implant. This pocket was made just slightly bigger than was needed for the implant. Once inserted and positioned two microscrews were used along the infraorbital rim for fixation. Eyelid closure consisted of cheeklift and orbicularis muscle suspension sutures as well as lateral canthopexies.
Under general anesthesia a lower eyelid incision was made 1mm below the lash line and stopping just at a vertical line dropped down from the pupil. From this limited eyelid incision approach, subperiosteal dissection as done over the entire footprint of the implant. This pocket was made just slightly bigger than was needed for the implant. Once inserted and positioned two microscrews were used along the infraorbital rim for fixation. Eyelid closure consisted of cheeklift and orbicularis muscle suspension sutures as well as lateral canthopexies.
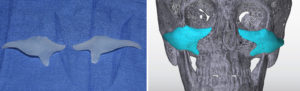
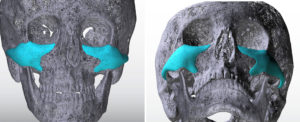 Custom infraorbital-malar implants provide an unparalleled ability to do what natural facial development did not. Its effectiveness ie because it is really an expansion of the natural bone surface in a confluent and connected design.
Custom infraorbital-malar implants provide an unparalleled ability to do what natural facial development did not. Its effectiveness ie because it is really an expansion of the natural bone surface in a confluent and connected design.
Case Highlights:
1) Infraorbital and anterior malar bone recession typically presents as lower eyelid bags, rim exposure and a negative orbital vector.
2) Skeletal correction ideally requires a bone augmentation approach using a custom implant design.
3) Custom infraorbital-malar implants are placed through a lower eyelid approach for optimal positioning.
Dr. Barry Eppley
Indianapolis, Indiana