


Background: Augmentation of the cheeks has been done almost as long as that of the chin. Historically done with implants and far more commonly today with synthetic fillers and fat. Besides the evolving methods to create a cheek augmentation effect, the aesthetic trends towards the desired cheek augmentation effect have also changed.
 For most women the desired cheek augmentation effect is a more anterior oval fullness involving the malar-submalar cheek areas. Some refer to this as an ‘apple cheek’ look, creating enhanced fullness below and around the primary cheek bone. (zygomatic body) It is important to note that some of this type of cheek augmentation is off of the bone, so it is really a combined hard and soft tissue type of facial augmentation. This is reflected in the different styles of cheek implants that are available today whose shapes are designed to augment various zones around this area.
For most women the desired cheek augmentation effect is a more anterior oval fullness involving the malar-submalar cheek areas. Some refer to this as an ‘apple cheek’ look, creating enhanced fullness below and around the primary cheek bone. (zygomatic body) It is important to note that some of this type of cheek augmentation is off of the bone, so it is really a combined hard and soft tissue type of facial augmentation. This is reflected in the different styles of cheek implants that are available today whose shapes are designed to augment various zones around this area.
 While this may be an aesthetic cheek augmentation desire for some women, it is almost never the desire for men who seek enhanced cheeks. The male goal is to have an enhanced cheekbone structure, making the existing cheekbones more visible. Anatomically this refers to the horizontal bone line from the infraorbital rim across the zygomatic body and back along the zygomatic arch. This form of skeletal cheek augmentation stays completely on the bone and, not surprisingly, is called the high cheekbone look. There may be different thicknesses or amounts of augmentation along this line based on patient preferences. Currently no standard cheek implant styles can create this midface effect.
While this may be an aesthetic cheek augmentation desire for some women, it is almost never the desire for men who seek enhanced cheeks. The male goal is to have an enhanced cheekbone structure, making the existing cheekbones more visible. Anatomically this refers to the horizontal bone line from the infraorbital rim across the zygomatic body and back along the zygomatic arch. This form of skeletal cheek augmentation stays completely on the bone and, not surprisingly, is called the high cheekbone look. There may be different thicknesses or amounts of augmentation along this line based on patient preferences. Currently no standard cheek implant styles can create this midface effect.

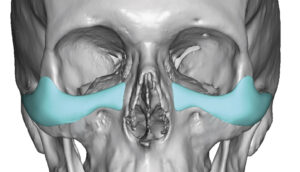
 Case Study: This male presented cheek augmentation to create the high cheek bone look.He also had some undereye hollows which was currency masked by injectable fillers. Using a 3D CT scan custom infraorbital-malar implants were designed with the intent of creating the high cheekbone look.
Case Study: This male presented cheek augmentation to create the high cheek bone look.He also had some undereye hollows which was currency masked by injectable fillers. Using a 3D CT scan custom infraorbital-malar implants were designed with the intent of creating the high cheekbone look.
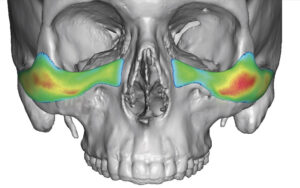
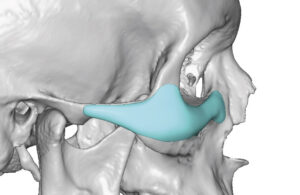
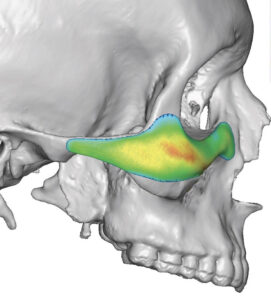 In design of such high cheekbone implants one can see that the entire implant runs along the skeletal line under the eye back towards the ear. The thickest part of the implant design is around the curvature of the cheeks in the Ogee curve location. It is this cheek area where the risk of being too big always exists as this is the where the greatest prominence of the implant’s projection exists.
In design of such high cheekbone implants one can see that the entire implant runs along the skeletal line under the eye back towards the ear. The thickest part of the implant design is around the curvature of the cheeks in the Ogee curve location. It is this cheek area where the risk of being too big always exists as this is the where the greatest prominence of the implant’s projection exists.

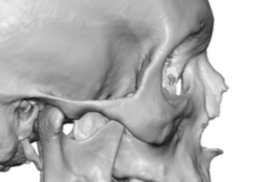
 Under general anesthesia and through a partial subciliary incision side subperiosteal undermining was done. The most challenging part is the dissection back along the zygomatic arch and the importance of getting past the mid-zygomatic suture which is usually at the maximum convexity of the arch. Besides the soft tissue adhesion to the suture the curve of the bone goes inward once past it and one must avoid continuing the dissection out into the overlying soft tissues. Staying on the bone with an elevator that has the right curve to it is the key to the arch dissection.
Under general anesthesia and through a partial subciliary incision side subperiosteal undermining was done. The most challenging part is the dissection back along the zygomatic arch and the importance of getting past the mid-zygomatic suture which is usually at the maximum convexity of the arch. Besides the soft tissue adhesion to the suture the curve of the bone goes inward once past it and one must avoid continuing the dissection out into the overlying soft tissues. Staying on the bone with an elevator that has the right curve to it is the key to the arch dissection.

 When trying in the implants it is important to assess the projection around the curve curve. It is extremely easy to overlook the strength of these prominence and assume every patient wants a very strong projection in his area. For many men less than 4mms is usually adequate. But when in doubt (which is often the case) leaves the design bigger in this area as it can always be reduced in surgery by a shaving technique. (which is frequently done)
When trying in the implants it is important to assess the projection around the curve curve. It is extremely easy to overlook the strength of these prominence and assume every patient wants a very strong projection in his area. For many men less than 4mms is usually adequate. But when in doubt (which is often the case) leaves the design bigger in this area as it can always be reduced in surgery by a shaving technique. (which is frequently done)
 Once positioned inside the lower eyelid and along the bone, one or two microscrews be used to secure it.
Once positioned inside the lower eyelid and along the bone, one or two microscrews be used to secure it.
custom infraorbital malar implants in a male Dr Barry Eppley IndianapolisThe high cheekbone look can only currently be achieved by a custom implant approach. There are a lot of variables to decide in the design for which there us no exact science in doing so. It takes a a lot of experience with these designs to learn what does and does not work well. Knowing how to get back along the zygomatic arch and place the implant through a limited lower eyelid incision while a avoiding after surgery lid abnormalities is a learned skill.
Case Highlights:
1) The high cheekbone look is created by making a horizontal augmentation line along the infraorbital rim back along he zygomatic arch.
2) Many custom infraorbital-malar implants are placed through a lower eyelid subciliary incisional approach which has the least risk of malpositioning.
3) The key dimensions in infraorbital-malar implants is its thickness as it turns the curve around the main cheekbone. (zygomatic body)
Dr. Barry Eppley
Indianapolis, Indiana