

Background: The undereye region of the midface is open to variable interpretations of what that is. As a result there are different terms that apply to describing undereye deficiency concerns of which tear troughs and hollows are the most commonly used. The anatomic basis for their appearance and how they can treated is, however, different.
A tear trough is a more localized term that applies to a discrete indentation along the infraorbital rim that is extremely common with aging. It indicates more of a soft tissue deficiency and not usually a bony one. It can be treated by a wide variety of approaches from injectable synthetic fillers and fat, orbital fat transposition, and various infraorbital rim onlay materials. Conversely, undereye hollows is a broader concept and can occur because of major fat loss with a normal bone structure. But more commonly it represents an underling skeletal deficiency of the infraorbital rim and often into the malar connection as well. The infraorbital rim is recessed and the entire lower eyelid region looks deficient. The key finding is that some degree of a negative orbital vector is present.
While all of the methods to treat tear troughs can be applied to undereye hollows they are less effective because of the broader surface area involvement of the problem. The more definitive treatment is to address the infraorbital rim deficiency. Standard tear trough implants can be helpful because they are dimensionally limited. They can not create an augmentation along the top of the infraorbital rim which is needed to optimally treat the orbital rim skeletal deficiency.
 Case Study: This thin young male was bothered by his undereye hollows. He had a narrow face and a a negative orbital vector on each side. Custom infraorbital-malar implants were placed through lower eyelid incisions.
Case Study: This thin young male was bothered by his undereye hollows. He had a narrow face and a a negative orbital vector on each side. Custom infraorbital-malar implants were placed through lower eyelid incisions.


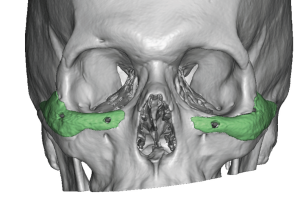
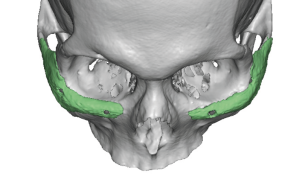 His before and after results shows the effects of the implants whose placement could be seen in a postoperative 3D CT scan.
His before and after results shows the effects of the implants whose placement could be seen in a postoperative 3D CT scan.
Undereye hollows that are associated with a skeletal deficiency are optimally treated by a custom implant approach whose surface area covers a significant part of the bony deficiency. With a negative orbital vector the bony deficiency is not just restricted to the infraorbital rim. It is the entire tripod complex that is recessed or, more accurately, rotated backwards. As a result the best anatomic correction is an augmentation along the infraorbital rim that extends up a bit onto the lateral orbital rim and anterior cheek. The more severe the deficiency the more the tripod legs of the implant needs to extend.
Case Highlights:
1) Undereye hollows can represent a bony deficiency of the infraorbital rim-malar complex.
2) In thin patients undereye hollows can only be permanently treated by infraorbital rim augmentation of which custom implants are one method of doing so.
3) Custom infraorbital rim-malar implants differ from standard tear trough implants in that they have broader surface area coverage and can saddle up over the rim.
Dr. Barry Eppley
Indianapolis, Indiana