

Background: Upper and lower jaw osteotomies, once known as orthognathic surgery, has undergone an evolution for what was its original purpose. Designed to correct dentofacial deformities for malocclusions, and while still used for that purpose today, its uses currently have expanded to the treatment of obstructive sleep apnea and as a method to increase mid- to lower facial projection for aesthetic purposes. One does not have to have a malocclusion to undergo the surgery and some patients do not even need orthodontic preparation for it.
Now known as Bimaxllary (Bimax) Advancements the primary movements are forward and often significantly so. While these facial bone movements have many benefits they can create a facial imbalance or disproportion. The facial bones above the LeFort 1 level are left behind so to speak and this can result in cheek and lower eye (infraorbital) deficiencies which are seen as lack of cheek projection and undereye hollows.
Unlike maxillary and mandibular bone movements through osteotomies there are no such anterior movement osteotomies for the orbits and cheeks. Augmentation can only be done by onlay augmentation of the bone with implants. And given the unique 3D shape of the orbits and cheeks custom designed implants are needed to achieve the proper effect.
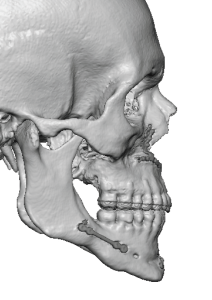
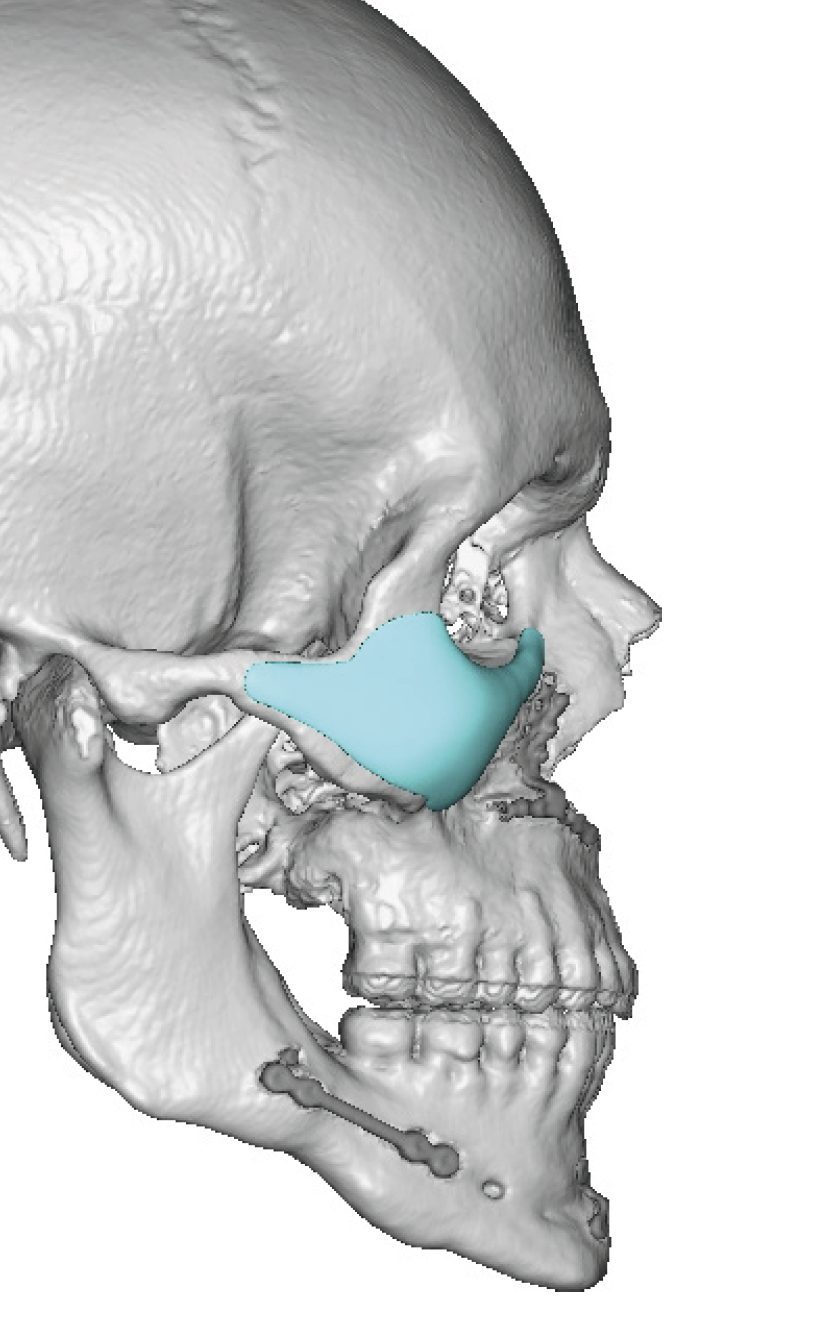
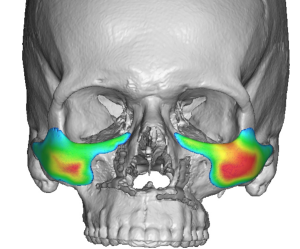
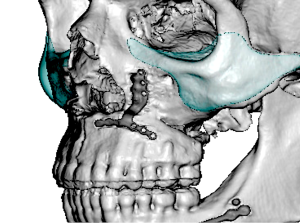
 Case Study: This male had a prior bimaxillary advancement procedure for sleep apnea which was 14mm forward. He probably always had some degree of infraorbital-malar hypoplasia but the large bimaxillary advancement and his thin face magnified the upper midface defieiency. His 3D CT showed the recessed infraorbital rim and cheekbone compared to the maxillomandibular complex beneath it.
Case Study: This male had a prior bimaxillary advancement procedure for sleep apnea which was 14mm forward. He probably always had some degree of infraorbital-malar hypoplasia but the large bimaxillary advancement and his thin face magnified the upper midface defieiency. His 3D CT showed the recessed infraorbital rim and cheekbone compared to the maxillomandibular complex beneath it.
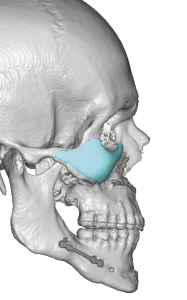
 Custom infraorbital-malar implants were designed with the consideration of his thin face so their projection was modest and not overly large to avoid creating an abnormal appearance.
Custom infraorbital-malar implants were designed with the consideration of his thin face so their projection was modest and not overly large to avoid creating an abnormal appearance.
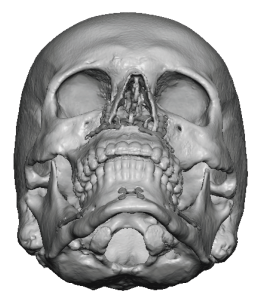
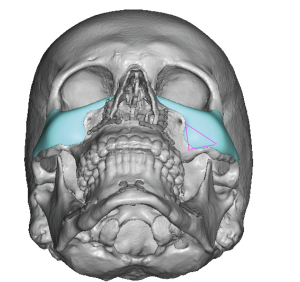
 There was some asymmetry with the left cheek needing more projection than that of the right. This asymmetry was clearly seen on the 3D CT scan in the submental view.
There was some asymmetry with the left cheek needing more projection than that of the right. This asymmetry was clearly seen on the 3D CT scan in the submental view.

 Under general anesthesia and through lower eyelid incisions the custom infraorbital-malar implants were placed and secured with a single microscrew.
Under general anesthesia and through lower eyelid incisions the custom infraorbital-malar implants were placed and secured with a single microscrew.
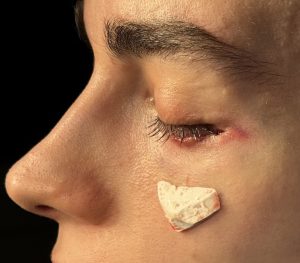
 On the left side even with the extra malar projection it still looked deficient so a carved ePTFE implant was placed as an overlay to the implant in that area.
On the left side even with the extra malar projection it still looked deficient so a carved ePTFE implant was placed as an overlay to the implant in that area.
 With bimaxillary advancements there is always the risk that the face above it will become deficient in projection. These risks are increased when the bimaxillary advancements are significant (8 to 10mms or greater) or if the patient has pre-existing lack of infraorbital-malar projection. (e.g., negative orbital vector) To avoid over correction or creating an unusual periorbital appearance the sizing of the infraorbital-malar implants must be carefully considered and in proportion with the shape of the overall face. In other words a large bimaxillary advancement doesn’t always mean large custom infraorbital-malar implants are needed.
With bimaxillary advancements there is always the risk that the face above it will become deficient in projection. These risks are increased when the bimaxillary advancements are significant (8 to 10mms or greater) or if the patient has pre-existing lack of infraorbital-malar projection. (e.g., negative orbital vector) To avoid over correction or creating an unusual periorbital appearance the sizing of the infraorbital-malar implants must be carefully considered and in proportion with the shape of the overall face. In other words a large bimaxillary advancement doesn’t always mean large custom infraorbital-malar implants are needed.
Key Points:
1) Significant bimaxillary advancements leaves the cheeks and infraorbital rims behind which in some patients may create an unbalanced facial appearance.
2) Custom infraorbital-malar implants provide projection to the upper midface to bring it into better balance with what was achieved at the LeFort I bone level.
3) The lower eyelid is the best incisional approach to provide proper placement of upper nidface implant placement with the lowest risk of complications.
Dr. Barry Eppley
World-Renowned Plastic Surgeon