

Background: Midface deficiencies are an interesting area of the face to augment as it is one of the few facial areas that has a significant concave shape to it. It also poses some anatomic issues with the prominent location of the infraorbital nerve. Traditionally midface augmentation was perceived as only being able to be effectively done by bone based procedures such as various Lefort osteotomies. But with a good occlusal relationship the only option are implants.
Midface implants have been historically thought of as standard shapes such as cheeks, infraorbital rim and paranasal-premaxillary styles. Patching these standard implants together is one approach to augment the midface but, in reality, creates an incomplete and uncontrolled augmentation result. Today the concept of a custom midface implant is the ideal treatment approach with a more complete and unified bony surface area coverage as well as preoperative control of implant thicknesses.
Many midface deficient patients receive some form of injectable volume augmentation albeit synthetic filler or fat. And while these treatments can produce positive improvements the effect is neither optimal or permanent. But their initial use can provide valuable information for custom midface implant designing, identifying the injectable augmentation locations and the volumes that were injected.
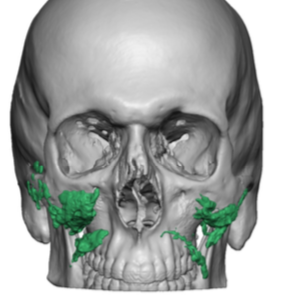
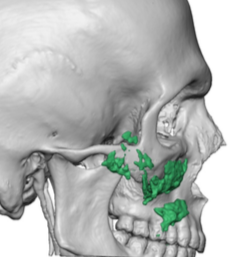
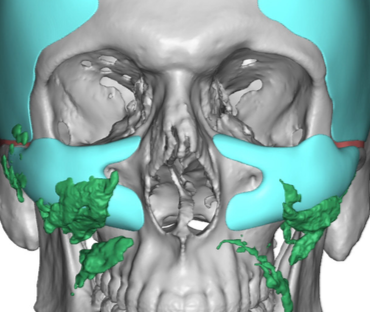
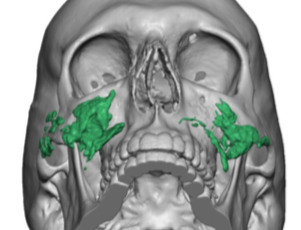 Case Study: This lean male with a thin face had been treating his midface deficiency with injectable fillers. But the volumes were never quite enough and filler fatigue can be an eventual issue for many patients. He decided to purse a more permanent solution with custom designed implants. His 3D CT scan showed the location of the injectable filler which was hydroxyapatite in composition (Radiesse) because of it being seen in the scan.
Case Study: This lean male with a thin face had been treating his midface deficiency with injectable fillers. But the volumes were never quite enough and filler fatigue can be an eventual issue for many patients. He decided to purse a more permanent solution with custom designed implants. His 3D CT scan showed the location of the injectable filler which was hydroxyapatite in composition (Radiesse) because of it being seen in the scan.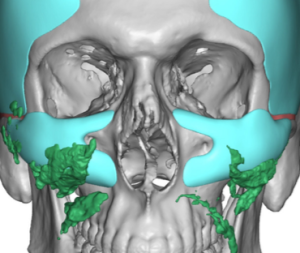
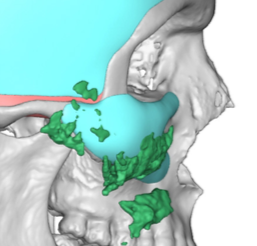
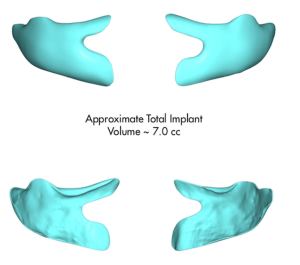 The location of the filler was very helpful in determining how the implant should be designed. While evaluating his face the infraorbital rim deficiency was evident but the filler shows how augmenting the midface below it was also important. A custom midface implant was designed that augmented the infraorbital rim, anterolateral zygoma and the concave surface of the maxilla. It essentially circled the infraorbital nerve excluding only the pyriform aperture region of the maxilla. It total volume was 7ccs per side. It is noted that he was also getting extended temporal implants which is not part of this case study.
The location of the filler was very helpful in determining how the implant should be designed. While evaluating his face the infraorbital rim deficiency was evident but the filler shows how augmenting the midface below it was also important. A custom midface implant was designed that augmented the infraorbital rim, anterolateral zygoma and the concave surface of the maxilla. It essentially circled the infraorbital nerve excluding only the pyriform aperture region of the maxilla. It total volume was 7ccs per side. It is noted that he was also getting extended temporal implants which is not part of this case study.


 The surgical placement of this type of custom midface implant (infraorbital-malar-maxillary implant) required a dual incisional approach. It is best when placing a combined convex-concave shaped implant that direct visualization is done for both differently shaped parts. This is particularly true when the infraorbital component of the implant is to provide vertical augmentation as well as the need to completely and safely encircle the infraorbital nerve. In addition screw fixation is needed at both the convex and concave levels of the implant.
The surgical placement of this type of custom midface implant (infraorbital-malar-maxillary implant) required a dual incisional approach. It is best when placing a combined convex-concave shaped implant that direct visualization is done for both differently shaped parts. This is particularly true when the infraorbital component of the implant is to provide vertical augmentation as well as the need to completely and safely encircle the infraorbital nerve. In addition screw fixation is needed at both the convex and concave levels of the implant.
Custom midface implants can provide an augmentation effect that supplants that of injectable fillers. They achieve this effect by overlaying most of the bony surface of the anterior midface from the infraorbital rim down as aesthetically needed. Their shape still follows the natural superior convex and inferior concave shape to the midface in varying amounts. They should almost always be placed with dual incisional visualization that assures the integrity of the infraorbital nerve.
Case Highlights:
1) Injectable fillers can be used to treat a midface deficiency but achieving a good augmentation effect may take considerable volume.
2) A 3D CT scan can be used to see hydroxyapatite fillers which can help in the design of a custom midface implant by their location and volume.
3) Placing a custom midface implant that encircles the infraorbital nerve and vertically augments the infraorbital rim requires a combined intraoral and lower eyelid incisions for proper implant placement.
Dr. Barry Eppley
Indianapolis, Indiana