

Background: Augmentation of aesthetic facial deformities are common procedures of which the lower third of the face (chin and jaw) is the most common. Augmentations of the upper two-thirds of the face is also done although lesser in number with the middle third of the face (cheeks, midface) being done more often than the upper third of the face. (forehead and brows) This is reflected in the implant augmentation options available for the chin, jaw angles, cheeks, nasal base and infraorbital rim.
There are autologous options for facial augmentations but they are limited in number as well as in their aesthetic effects. The most well known is the sliding genioplasty which can be a good alternative to a chin implant in many cases when horizontal and vertical dimensional changes are needed. Cheek osteotomies are also available but their aesthetic effect is limited to widening of the zygomatic body only.
When it comes to the upper midface (infraorbital-malar-maxillary) an autologous option exists known as a modified LeFort III osteotomy. By diagram this looks appealing and is performed through combined intraoral and lower eyelid incisions. It is called a modified LeFort III as it does not cross the nose in the midline and are separately performed bilateral osteotomies. While it avoids the use of implants it only permits a limited amount of movement of a few millimeters in any dimension. If this proves inadequate secondary implant augmentation is the salvage procedure.
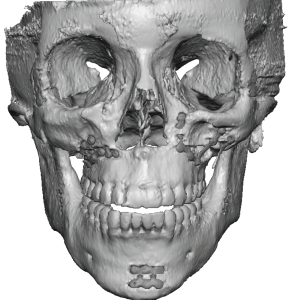
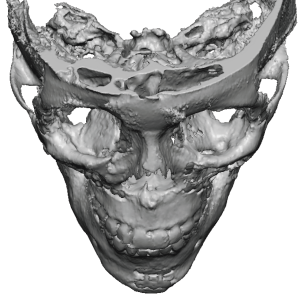 Case Study: This female had infraorbital-malar deficiency (hollow undereyes with flat cheeks) and had a modified LeFort III procedure performed. While she liked the effect when the tissues were swollen eventually when the final result appeared she saws minimal difference/improvement. Her 3D CT scan showed the numerous fixation plates and the ZMC osteotomy lines but the actual forward bony movement appeared to be minimal.
Case Study: This female had infraorbital-malar deficiency (hollow undereyes with flat cheeks) and had a modified LeFort III procedure performed. While she liked the effect when the tissues were swollen eventually when the final result appeared she saws minimal difference/improvement. Her 3D CT scan showed the numerous fixation plates and the ZMC osteotomy lines but the actual forward bony movement appeared to be minimal.
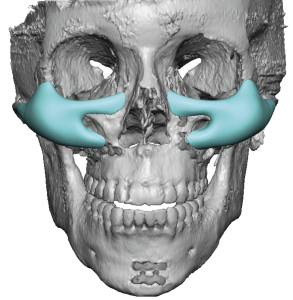
 A custom infraorbital-malar-maxillary midface implant was designedback of the head skull implant was designed with 8mm malar projection and a saddling of the infraorbital rim. The total implant volumes were 7ccs per side.
A custom infraorbital-malar-maxillary midface implant was designedback of the head skull implant was designed with 8mm malar projection and a saddling of the infraorbital rim. The total implant volumes were 7ccs per side.
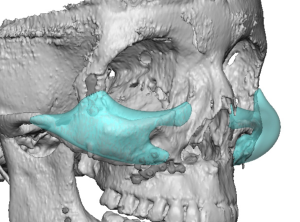
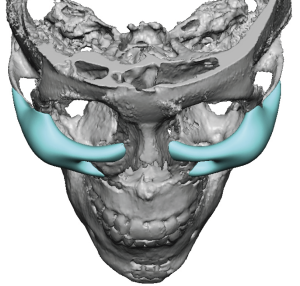
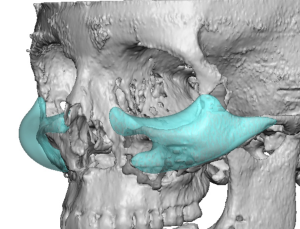 In the oblique views the change in the upper midface projection (Ogee curve) could be appreciated.
In the oblique views the change in the upper midface projection (Ogee curve) could be appreciated.

 Under general anesthesia and through combined existing lower eyelid and intraoral scars, the midface tissues were elevated to permit implant placement.
Under general anesthesia and through combined existing lower eyelid and intraoral scars, the midface tissues were elevated to permit implant placement.

 Microscrew fixation was done at both the medial and lateral infraorbital rim.
Microscrew fixation was done at both the medial and lateral infraorbital rim.
While the appeal of using your own bone (tissues) for an aesthetic facial augmentation is understandable their aesthetic effects are often limited. But for those so motivated an osteotomy approach is usually safe and has few complications. But if inadequate aesthetic results are obtained a secondary custom implant approach offers a definitive multi-dimensional expansion of the undereye and cheek areas.
Key Points:
1) Upper midface augmentation of the infraorbital-malar bones can theoretically be done by skeletal advancement (modified LeFort III osteotomy) but is a challenging procedure in an aesthetic application.
2) When a modified LeFort III procedure proves inadequate only augmentation with a custom midface implant design is a more effective aesthetic procedure.
3) Dual access via the lower eyelid and intraoral incisions is needed to properly placed this type of custom midface implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon