

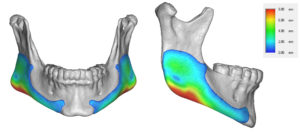
Background: The shape of the lower jaw is influenced by a variety of genetic bone growth and postnatal musculoligamentous attachments. This is most evident in the high jaw angle patient who, by definition, has a steep mandibular plane angle. What is often noted in their 3D CT scans is the bony exostoses that exist along the jaw angles and a more pronounced antegonial notch.
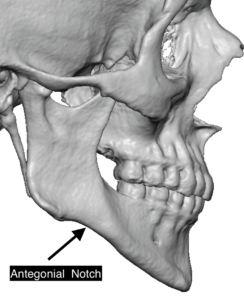
The antegonial notch is a well known feature of the jawline that exists between the jaw angle and the mandibular body. Its presence and extent varies widely Its existence/purpose can be debated but its smooth and upwardly curved shape indicates this is where the masseter muscle is not. This can be confirmed surgically when placing custom jawline implants where the subperiosteal dissection is loosely attached and the fatty tissue beneath the jawline is easily seen.
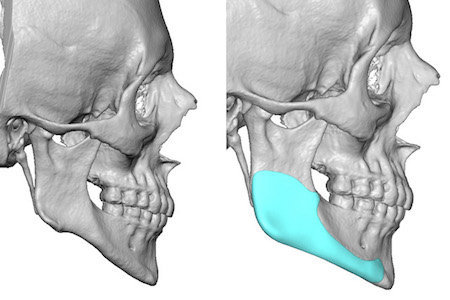
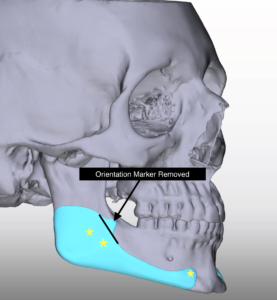
 The depth of the antegonial notch and the disruption of a smooth jawline always exists in the high jaw angle patient. The attachment and pull of the masseter muscle creates the raised rim of bone and ‘bumps’ around the jaw angle. The absence of any masseter muscle attachments leaves a smooth and upwardly curved jawline in front of the angle. When creating an improved jawline in these patients the custom implant design must drop down the jaw angle and fill in the antegonial notch as the design extends forward to the chin.
The depth of the antegonial notch and the disruption of a smooth jawline always exists in the high jaw angle patient. The attachment and pull of the masseter muscle creates the raised rim of bone and ‘bumps’ around the jaw angle. The absence of any masseter muscle attachments leaves a smooth and upwardly curved jawline in front of the angle. When creating an improved jawline in these patients the custom implant design must drop down the jaw angle and fill in the antegonial notch as the design extends forward to the chin.
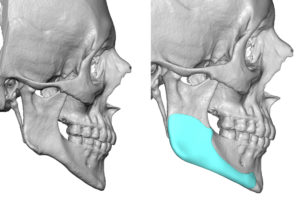
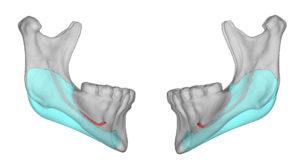
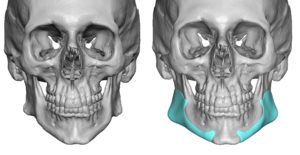 Case Study: This male desired a jawline reshaping implant that corrected his high jaw angles and filled in what appeared to be ‘missing’. In some ways this is almost a reconstructive implant to restore a jawline that is congenitally deficient. Instead of correcting the typical jaw deformity of lack of chin projection this was correcting the deficiency at the back part of the jaw. Using his 3D CT scan custom jaw angle implants were designed to fill in the missing part of the posterior jawline from the angles to the chin. This type of jawline implant just extend all the way to the chin to create a smooth jawline. It is also important to not add too much width as the vertical lengthening effects alone adds a a certain amount of width by itself.
Case Study: This male desired a jawline reshaping implant that corrected his high jaw angles and filled in what appeared to be ‘missing’. In some ways this is almost a reconstructive implant to restore a jawline that is congenitally deficient. Instead of correcting the typical jaw deformity of lack of chin projection this was correcting the deficiency at the back part of the jaw. Using his 3D CT scan custom jaw angle implants were designed to fill in the missing part of the posterior jawline from the angles to the chin. This type of jawline implant just extend all the way to the chin to create a smooth jawline. It is also important to not add too much width as the vertical lengthening effects alone adds a a certain amount of width by itself.


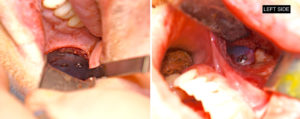
 Under general anesthesia and through a completely intraoral approach (one anterior and bilateral posterior vestibular incisions), the custom jaw angle implants were placed with double screw fixation at the jaw angles and single screw fixation at the chin placement tab.
Under general anesthesia and through a completely intraoral approach (one anterior and bilateral posterior vestibular incisions), the custom jaw angle implants were placed with double screw fixation at the jaw angles and single screw fixation at the chin placement tab.
 An important key when the jaw angle is vertically lengthened by an implant is to carefully release the masseter muscle attachments around the angular bone. Strong ligamentous attachments can the expected when bony exostoses or bumps are seen on the 3D CT scan prior to surgery. Aggressive or overzealous subperiosteal elevation along the inferior border of the jaw angle can result in masseter muscle dehiscence and implant show.
An important key when the jaw angle is vertically lengthened by an implant is to carefully release the masseter muscle attachments around the angular bone. Strong ligamentous attachments can the expected when bony exostoses or bumps are seen on the 3D CT scan prior to surgery. Aggressive or overzealous subperiosteal elevation along the inferior border of the jaw angle can result in masseter muscle dehiscence and implant show.
 Correction of the steep mandibular plane angle and filling in the accentuated antegonial notch requires an implant design that extends all the way to the chin to achieve a smooth jawline. The extension to the chin can be placed and secured through either an intraoral or submental approach which would affect the shape of the ned of the implant.
Correction of the steep mandibular plane angle and filling in the accentuated antegonial notch requires an implant design that extends all the way to the chin to achieve a smooth jawline. The extension to the chin can be placed and secured through either an intraoral or submental approach which would affect the shape of the ned of the implant.
Case Highlights:
1) The high jaw angle patient has a steep mandibular plane angle which can be associated with a normal horizontal chin position.
2) A deep antegonial notch can be occasionally seen in the high jaw angle/steep mandibular plane angle patient.
3) A custom jaw angle implant design must concurrently lower the jaw angle, fill in the antegonial notch and create a smooth jawline up to the chin.
Dr. Barry Eppley
Indianapolis, Indiana