

Background: Custom jawline implants provide a unique and most powerful effect on the lower face due to their wrap around designs. Extending from one jaw angle to the other they create a change to the complete inferolateral border of the lower jaw. Of the five parts of the lower jaw (symphysis, body and ramus) the most challenging part of their designs is what is done at the ramus. (jaw angles) Besides being a paired part of the lower jaw they are unique from the rest of the implant design due to their envelopment by the masseter muscles.
The masseter muscle had a broad origin along the zygomatic arch and cheekbone and narrows down in a triangular shape to its insertion over the jaw angles at the intersection of its posterior and inferior borders. It attaches through ligaments which are clearly discernible in jaw angle implant surgery and these must be considered both in implants design as well as how they are manipulated during surgery.
As has been learned from looking at thousands of 3D CT scans from custom implant designs the masseter muscle ligamentous attachments are often visible. They appear as bony bumps at and anterior to the jaws angle point. Men almost always have them in varying prominences and in women they are often barely visible or are not present at all. They indicate both the strength of the ligamentous attachments as well as how easy or difficult it would be to elevate them off of the bone…an essential component of the successful placement of both standard jaw angle implants and custom jawline implants.
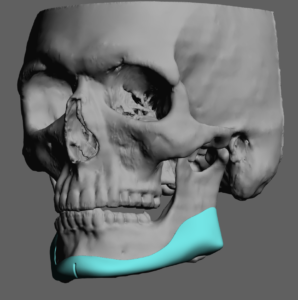
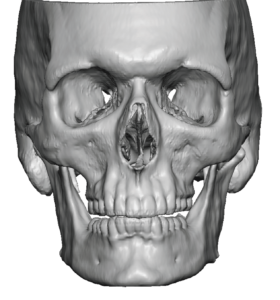 Case Study: This male presented for a custom jawline implant and a desire for stronger jaw angle appearance. He had a naturally broader lower facial appearance with large strong massager muscles. His 3D CT scan showed three distinct bony bumps along the jaw angles in the side view. In the front view these bony bumps appeared as discernible projections from the jaw angles indicating how pronounced they were. As would be expected from his wide lower facial appearance the scan shows how strong these ligamentous attachments were which is consistent with large masseter muscles in a male.
Case Study: This male presented for a custom jawline implant and a desire for stronger jaw angle appearance. He had a naturally broader lower facial appearance with large strong massager muscles. His 3D CT scan showed three distinct bony bumps along the jaw angles in the side view. In the front view these bony bumps appeared as discernible projections from the jaw angles indicating how pronounced they were. As would be expected from his wide lower facial appearance the scan shows how strong these ligamentous attachments were which is consistent with large masseter muscles in a male.
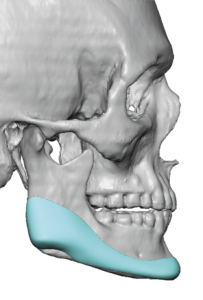
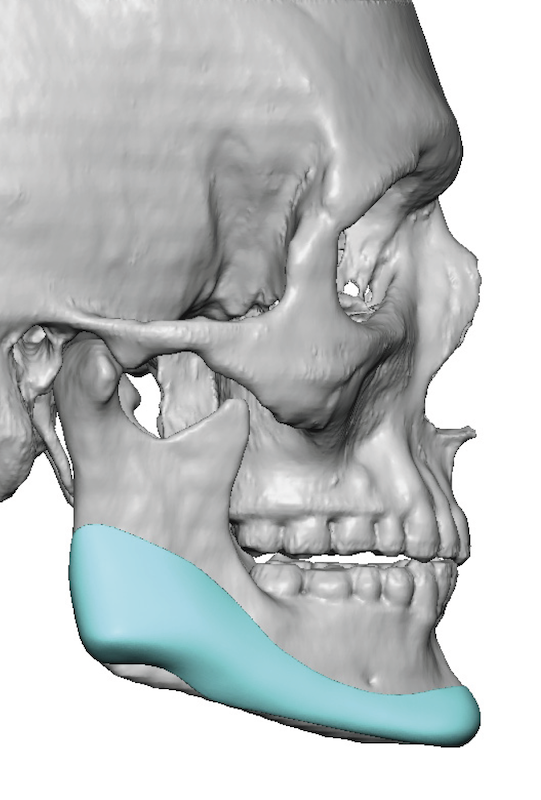
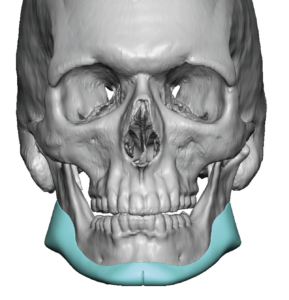 His custom jawline implant was designed to only add width at the jaw angles. But in so doing it was designed around the ligamentous attachments so they would not have to be elevated and risk postoperative muscle dehiscence. Not releasing the strong attachments should not interfere with getting tiger desired with since the implant design pushes out on the muscle everywhere else on the ramus.
His custom jawline implant was designed to only add width at the jaw angles. But in so doing it was designed around the ligamentous attachments so they would not have to be elevated and risk postoperative muscle dehiscence. Not releasing the strong attachments should not interfere with getting tiger desired with since the implant design pushes out on the muscle everywhere else on the ramus.


 Under general anesthesia and a combined submental and intraoral posterior vestibular incisions the custom jawline implant was placed. In looking at the implant during surgery the ligamentous reliefs (notches) on the jaw angle portion of the implant can be clearly seen.
Under general anesthesia and a combined submental and intraoral posterior vestibular incisions the custom jawline implant was placed. In looking at the implant during surgery the ligamentous reliefs (notches) on the jaw angle portion of the implant can be clearly seen.
 One of the known, but often underappreciated, risks of placing any implant at the jaw angles is masseteric muscle dehiscence. This is the direct result of release of the ligamentous attachments and subsequent muscle retraction. Just because the ligaments are elevated does not always mean the muscle will retract. But if the implant design vertically lengthens the jaw angles that potential risk is increased. But when only width is added to the jaw angles one method when strong ligamentous attachments are present is to design the implants around them.
One of the known, but often underappreciated, risks of placing any implant at the jaw angles is masseteric muscle dehiscence. This is the direct result of release of the ligamentous attachments and subsequent muscle retraction. Just because the ligaments are elevated does not always mean the muscle will retract. But if the implant design vertically lengthens the jaw angles that potential risk is increased. But when only width is added to the jaw angles one method when strong ligamentous attachments are present is to design the implants around them.
Case Highlights:
1) Two-thirds of a custom jawline implant design is at the jaw angles.
2) The ligamentous attachments of the masseter muscle are directly over the jaw angle region of the implant can can be adversely affected by its design.
3) In width only jawline implant designs at the jaw angles a relief in the design can be done when strong ligamentous attachments are present.
Dr. Barry Eppley
World-Renowned Plastic Surgeon