

Background: Orthognathic surgery, whether it involves one jaw or two, can produce some phenomenal results from an external facial appearance. The more under projected the lower face is, setting the occlusion into the desired position in space can create substantial improvements in the outward facial appearance as the facial bones follow around it.
But despite the substantial facial changes that some orthognathic surgery patients achieve, the operation does have its limitations in some bony dimensions. It is a primarily a horizontally projecting operation with some vertical changes possible in the upper jaw but not very much in the lower jaw. It is also very limited for what it can accomplish in width usually creating little to no width in either the upper or lower jaw in particular.
As a result of these dimensional movement limitations as well as bony changes that are well known to occur around the sagittal split ramus osteotomy site, the lower jaw can remain aesthetically deficient in some patients. Once the bone of the lower jaw has been relocated only augmenting its entire external contour can produce a complementary additional three-dimensional enhancement.
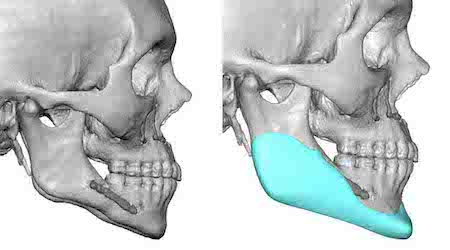
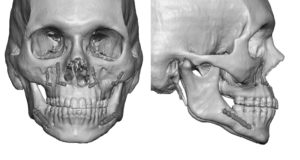 Case Study: This male had been through a successful bimaxillary orthognathic surgery procedure. While he was happy with his occlusion he felt his lower still lack projection as well as width. 3D CT scan assessment showed that the lower jaw was vertically deficient from angle to chin as well as remans with some modest horizontal deficiency in the side profile view. Frontally the entire jawline was narrow with an inward V-shape between the zygomatic arches and the lateral jawline.
Case Study: This male had been through a successful bimaxillary orthognathic surgery procedure. While he was happy with his occlusion he felt his lower still lack projection as well as width. 3D CT scan assessment showed that the lower jaw was vertically deficient from angle to chin as well as remans with some modest horizontal deficiency in the side profile view. Frontally the entire jawline was narrow with an inward V-shape between the zygomatic arches and the lateral jawline.

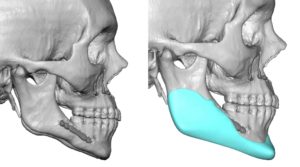
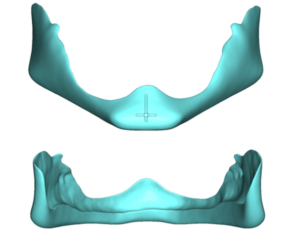
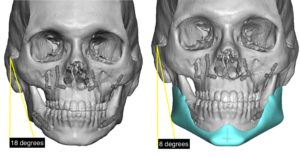 Using his 3D CT scan a custom jawline implant was designed that provided the desired vertical lengthening along the entire jawline as well as 7mms of horizontal chin projection. The combination of the 7mms of horizontal chin projection and 7mms of vertical chin lengthening was at the maximum (collectively 14mms) that the soft tissue chin pad can successfully redraw over an implant. In the front view the added width of the jaw angle produced a reduction of ten degrees in the zygomatic arch-gonial angle.
Using his 3D CT scan a custom jawline implant was designed that provided the desired vertical lengthening along the entire jawline as well as 7mms of horizontal chin projection. The combination of the 7mms of horizontal chin projection and 7mms of vertical chin lengthening was at the maximum (collectively 14mms) that the soft tissue chin pad can successfully redraw over an implant. In the front view the added width of the jaw angle produced a reduction of ten degrees in the zygomatic arch-gonial angle.


 Under general anesthesia the custom jawline implant was introduced in a front to back one-piece technique through the submental incision.
Under general anesthesia the custom jawline implant was introduced in a front to back one-piece technique through the submental incision.
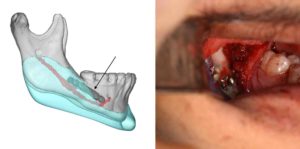
 Positioning of the jaw angle portion of the implant, which is always the hardest part of any jawline implant placement, was aided by the known location of the implant over the indwelling sagittal split fixation plate and screws. The other design feature that helps with intraoperative positioning of the implant is that the entire inferior border fits into a channel on the inside of the implant, a design feature unique to vertically lengthening jawline implants.
Positioning of the jaw angle portion of the implant, which is always the hardest part of any jawline implant placement, was aided by the known location of the implant over the indwelling sagittal split fixation plate and screws. The other design feature that helps with intraoperative positioning of the implant is that the entire inferior border fits into a channel on the inside of the implant, a design feature unique to vertically lengthening jawline implants.
Case Highlights:
1) Orthognathic surgery largely provides horizontal and vertical jawline changes but not width.
2) A custom jawline implant can complement a prior orthognathic surgery procedure by providing increased three-dimensional enhancement of the lower jaw.
3) The existing plates and screws from the mandibular osteotomy can serve as intraoperaive registration for jawline implant placement.
Dr. Barry Eppley
Indianapolis, Indiana