

Background:
Double jaw osteotomy surgery is very popular today for multiple reasons. Several of the reasons for the surgery today are quite different than they were two or three decades ago. While once reserved primarily for the correction of malocclusions the treatment of obstructive sleep apnea as well as for aesthetic purposes has expanded the number of patients undergoing double jaw surgery. Despite its many benefits, double jaw surgery can have minor aesthetic drawbacks. The most common would be the disruption of an otherwise smooth bony inferior border of the lower jaw as well as alterations in the facial shape and proportions.
As a result of its increased popularity, particularly for its aesthetic benefits, some of these aesthetic drawbacks may not be so minor to some patients. The combination of bony inferior border irregularities, the desire for a more three dimensional jaw augmentation effect and correction of some asymmetries lead patients to consider a custom jawline implant. This is the only method to comprehensively address these concerns in a preoperatively planned process.
In designing custom jawline implants after double jaw surgery common questions and considerations are whether the existing hardware needs to be removed and whether it can be combined with other concurrent jaw procedures. The consideration of the hardware is that overlying the sagittal split area and that never needs to be preoperatively removed. Conversely having it present helps with the implant design and can be a very important intraoperative guide as to how to properly position the jawline implant. The jawline implant can also be done with concurrent bony chin procedures regardless of those dimensional changes needed and can be factored into the implant design process.
Case Study:
This young male presented with a complex history of double jaw and chin surgeries. He originally had double jaw surgery combined with a vertical lengthening bony genioplasty. This was complicated by a nonunion of the right sagittal split site which required two additional surgeries for bony consolidation. The results of these multiple site osteotomies resulted in numerous jawline inferior border bony irregularities. In addition, and more importantly, aesthetically he was left with a very high jaw angle shape which was magnified by his prior vertical lengthening bony genioplasty. His goals now were for a more aesthetically pleasing jaw shape which would consist of a vertical chin shortening and some modest lengthening of the jawline behind it. As part of that correction smoothing out the inferior border of the lower jaw from one angle to the other as well as correction of some asymmetry was also desired.
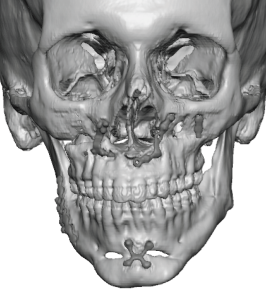
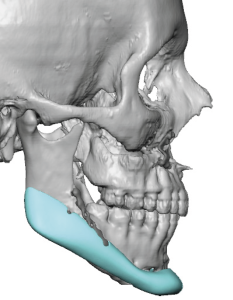
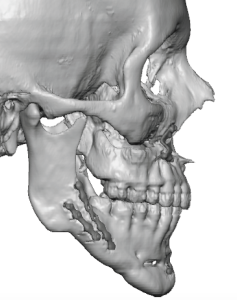 His 3-D CT scan demonstrated all of the above bone shape problems as well as the very steep mandibular plane angle that resulted from these prior surgeries.
His 3-D CT scan demonstrated all of the above bone shape problems as well as the very steep mandibular plane angle that resulted from these prior surgeries.
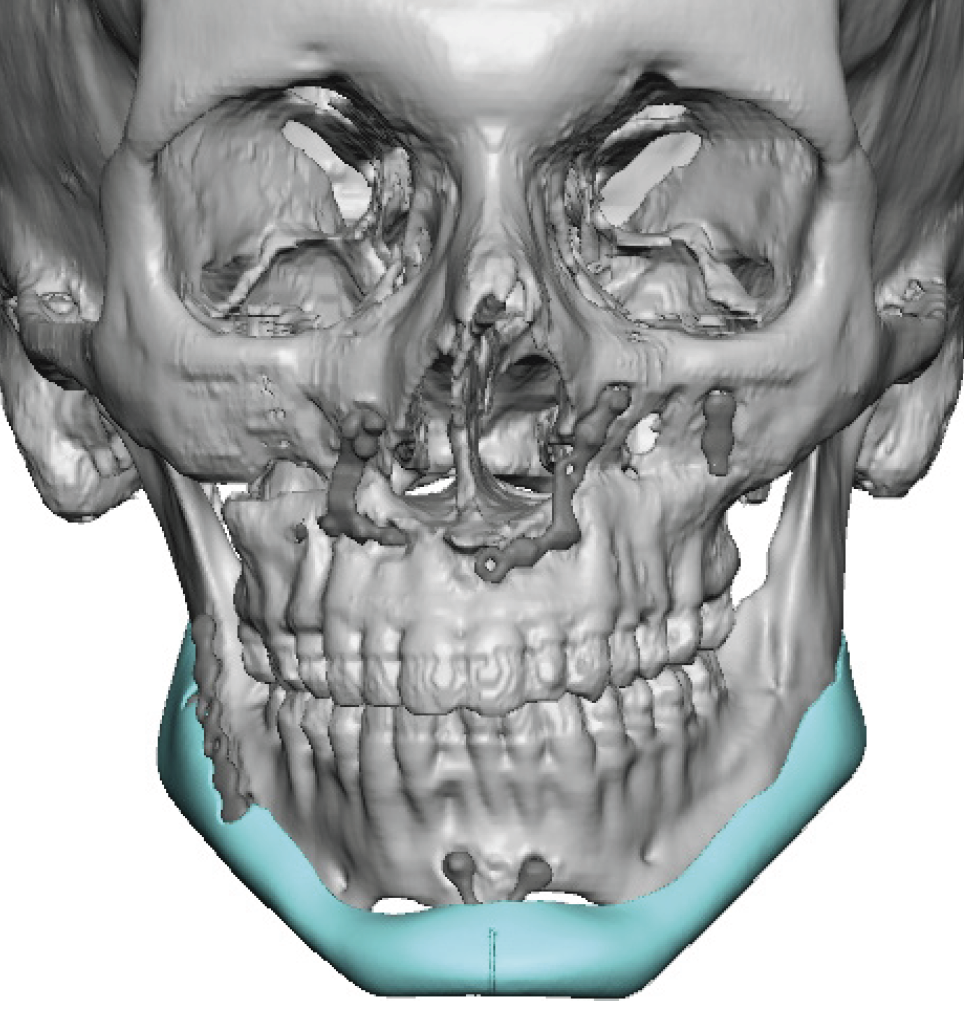
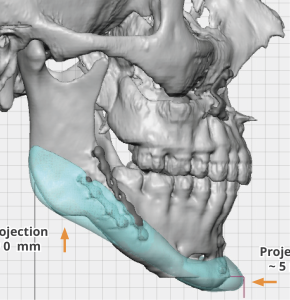
 A custom jawline implant was designed for these corrections and it was to be combined with a vertical shortening bony genioplasty. As part of the surgical plan he did not want any external incisions so a three incisional intraoral approach was planned.
A custom jawline implant was designed for these corrections and it was to be combined with a vertical shortening bony genioplasty. As part of the surgical plan he did not want any external incisions so a three incisional intraoral approach was planned.
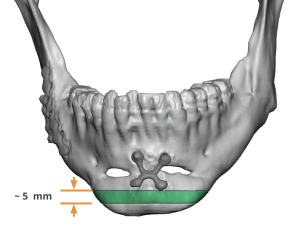 The vertical reduction of the bony chin must be factored into the implant design. This is done in a digital fashion before the implant design is done around it. In his case the bony reduction was 5 mm which probably was similar to the amount of vertical lengthening that was initially done.
The vertical reduction of the bony chin must be factored into the implant design. This is done in a digital fashion before the implant design is done around it. In his case the bony reduction was 5 mm which probably was similar to the amount of vertical lengthening that was initially done.
Under general anesthesia the first procedure was a 5 mm vertical chin reduction removing a wedge of bone after plate and screw removal. The bone was then re-secured in a vertically shorter position with a single plate and screws.

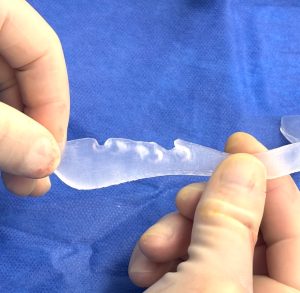

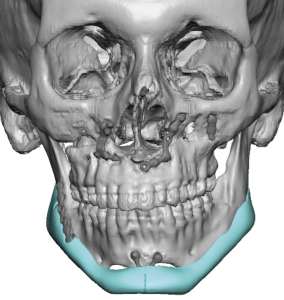
 The custom jawline implant was opened and one feature of it, as planned in the design, was using the sagittal split hardware as a registration for the placement of the back part of the implant. As an be seen on the implant there is a plate relief for the lower sagittal split plate.
The custom jawline implant was opened and one feature of it, as planned in the design, was using the sagittal split hardware as a registration for the placement of the back part of the implant. As an be seen on the implant there is a plate relief for the lower sagittal split plate.
The custom jawline implant was then successfully placed through the chin reduction osteotomy site aided by additional posterior intraoral vestibular incisions. The back part of the implant was secured to the inferior sagittal split osteotomy plate by removal of some of its screws with new screws inserted through the implant and plate to the bone.
 While a smooth bony contour is not typically perceived as a dimensional component of the mandible tt is the fourth dimension of lower facial aesthetics. We take the smooth contour of the inferior border of the lower jaw for granted until it becomes disruptive by surgery. In some cases these bony irregularities are easily seen while in others it is more palpable. But when the bony regularities are combined with asymmetries and the desire for a more three dimensional augmentation effect, subtle as they may be, the relevance of a custom jawline implant comes into play. The greatest bony irregularities are usually in the into the antegonial area at the anterior jaw angles. Many patients have an existing antegonial notch which often becomes magnified after a sagittal split osteotomy. Creating a smooth inferior border of the lower jaw is usually most needed in this area.
While a smooth bony contour is not typically perceived as a dimensional component of the mandible tt is the fourth dimension of lower facial aesthetics. We take the smooth contour of the inferior border of the lower jaw for granted until it becomes disruptive by surgery. In some cases these bony irregularities are easily seen while in others it is more palpable. But when the bony regularities are combined with asymmetries and the desire for a more three dimensional augmentation effect, subtle as they may be, the relevance of a custom jawline implant comes into play. The greatest bony irregularities are usually in the into the antegonial area at the anterior jaw angles. Many patients have an existing antegonial notch which often becomes magnified after a sagittal split osteotomy. Creating a smooth inferior border of the lower jaw is usually most needed in this area.
Highlights:
1) Bony jawline irregularities are not uncommon after sagittal split and chin osteotomies.
2) The only way to smooth out irregular jawline successfully is with the custom jawline implant design. This also provides the opportunity for any other three dimensional aesthetic augmentations that the patient desires.
3) A custom jawline implant can be combined with a vertical reduction genioplasty and can be done completely intraorally.
Dr. Barry Eppley
World-Renowned Plastic Surgeon