


Background: There are two basic autologous methods of changing the shape/position of the lower jaw. The sagittal split ramus osteotomy (SSRO) moves the body and symphysis bone while the sliding genioplasty (SG) repositions the symphysis (chin) bone. Both do so by cutting through the entire vertical length of the involved jaw bone done through its inferior border. The inferior border is the thick smooth edge that runs along the entire jawline from side to side that one commonly feels with their hand.
When the bones are moved and put back together in a new position there is always going to be some contour disruption of the inferior border. The only question is how significant will they be. This inferior border disruption is well recognized in the sliding genioplasty procedure and is known as ‘stepoffs’ which, when significant, can be seen externally as soft tissue indentations over them. Less recognized is what can occur with the SRRO procedure in which the shape of the entire jaw angle can change with irregularities or becoming vertically shorter particularly in large Bimax movements.
When a BSSO and a SG are performed together there is a potential for four different locations of disruption of the inferior border of the lower jaw. Smoothing out the jawline after such orthognathic surgery can only be done with a custom jawline implant with the benefits that any other aesthetic dimensional augmentation changes can be done at the same time.

 Case Study: This male had a prior double jaw surgery for obstructive sleep apnea with a 10mm Bimax advancement. While very effective for his sleep apnea correction he had residual jaw angle deformities, a desire for improved jaw angle definition and palpable implants that had been concurrently placed around his chin area. The indentations in his jaw angle area were evident externally particularly on the right side.
Case Study: This male had a prior double jaw surgery for obstructive sleep apnea with a 10mm Bimax advancement. While very effective for his sleep apnea correction he had residual jaw angle deformities, a desire for improved jaw angle definition and palpable implants that had been concurrently placed around his chin area. The indentations in his jaw angle area were evident externally particularly on the right side.

 His 3D CT scan showed the prominent irregularities along his jawline at the chin and jaw angle areas. The inferior border disruption on the right side was the most significant of the two sides due to an over rotation of the proximal ramus segment as it was put together with the distal segment. There was also an implant shadow and screws visible across the chin area consistent with his knowledge of Medpor implants being added to the chin area during the surgery.
His 3D CT scan showed the prominent irregularities along his jawline at the chin and jaw angle areas. The inferior border disruption on the right side was the most significant of the two sides due to an over rotation of the proximal ramus segment as it was put together with the distal segment. There was also an implant shadow and screws visible across the chin area consistent with his knowledge of Medpor implants being added to the chin area during the surgery.
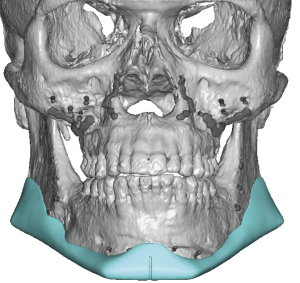
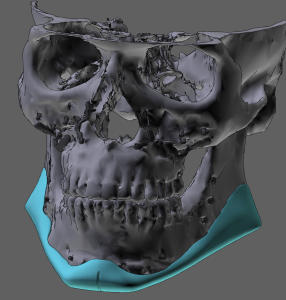
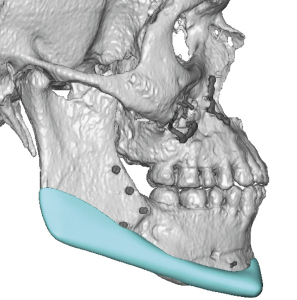 A custom jawline implant was designed to smooth out the inferior border, provide augmentation and shape to the jaw angles and provide minimal/negligible augmentation to the chin.
A custom jawline implant was designed to smooth out the inferior border, provide augmentation and shape to the jaw angles and provide minimal/negligible augmentation to the chin.
 Under general anesthesia and through his three existing incisions (submental and posterior intraoral) the Medpor implants were identified and removed. This then cleared the way for the dissection and placement of the custom jawline implant.
Under general anesthesia and through his three existing incisions (submental and posterior intraoral) the Medpor implants were identified and removed. This then cleared the way for the dissection and placement of the custom jawline implant.
 A custom jawline implant can be used to smooth out an irregular jawline without adding much volume/augmentation to jaw areas that don’t need it. In this case he didn’t need any chin augmentation effect so minimal material was placed there, just enough to add some width to the chin and the jawline behind it. It is the jaw angles that needed and received the largest volume of the implant material.
A custom jawline implant can be used to smooth out an irregular jawline without adding much volume/augmentation to jaw areas that don’t need it. In this case he didn’t need any chin augmentation effect so minimal material was placed there, just enough to add some width to the chin and the jawline behind it. It is the jaw angles that needed and received the largest volume of the implant material.
Key Points:
1) All osteotomies of the lower jaw, sagittal split ramus osteotomies and sliding genioplasties, have the potential to leave inferior border jawline irregularities.
2) Custom jawline implants can be used to smooth out the irregular inferior border without creating any significant jaw augmentation effect.
3) Previously placed materials, like Medpor, that have been used to try and smooth out jaw irregularities can be removed with the custom jawline implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon