

Background: A custom jawline implant has a total reshaping effect on the lower third of the face. It does so by virtue of its surface area coverage with a complete augmentation of the entire inferolateral surface of the lower jaw from angle to angle. This makes it the biggest type of facial implant that can be placed by both surface area and volume. (such implant volumes range for 8 to 27 ccs)
Healing of the total jawline implant occurs by an expected biologic response which is isolation from the surrounding tissues through scar encapsulation. This is what occurs with any implant placed in the body whether it is for medical purposes or just for aesthetic enhancement. What is unique about jawline implants, which is well known from chin implant experience, is that bone overgrowth can and often does occur. It is seen most consistently at the jaw angles where it is much more robust than ever seen in chin implants. Due to the elevation of the periosteum and the thick masseter muscle a generous osteogenic response occurs. This typically covers the superior border of the implant, and if one is unaware of this osteogenic response, may to be able to ‘find’ the implant.
These typical biologic reactions around a custom jawline implant has great relevance when re-entering the implantation site. This is most commonly done in replacement surgery when the patient has decided they have a better implant design after seeing what the initial implant aesthetically accomplished. While one would think that such a decision is a rare occurrence, it is actually not.
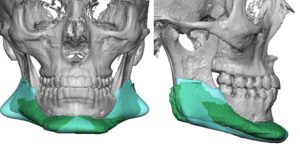
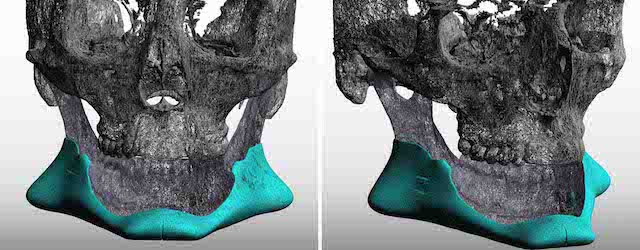
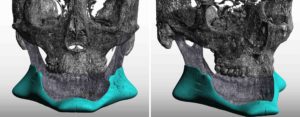
 Case Study: This male had a custom jawline implant placed once year previously. While he had major improvement he concluded that he wanted a new implant that had less chin and connector width and more jaw angle width. A new 3D CT scan was done to confirm the symmetric placement of the implant so designing around it could be 100% accurately done. The new implant (in teal blue) is overlaid on the indwelling implant (in green) so their different effects could be seen.
Case Study: This male had a custom jawline implant placed once year previously. While he had major improvement he concluded that he wanted a new implant that had less chin and connector width and more jaw angle width. A new 3D CT scan was done to confirm the symmetric placement of the implant so designing around it could be 100% accurately done. The new implant (in teal blue) is overlaid on the indwelling implant (in green) so their different effects could be seen.
 Under general anesthesia and through his well healed submental skin and bilateral intraoral incisions, his existing implant was removed by sectioning it into multiple pieces. The size of the chin and jaw angles made this necessary as they could not be slid through the much smaller and tightly scarred pocket tunnel between the two. Given this expected observation the new implant was split into two pieces and placed in a back to front direction and reunited in the middle of the chin. (In some cases the unique internal wedge design on the jaw angles may permit it to be placed as one piece)
Under general anesthesia and through his well healed submental skin and bilateral intraoral incisions, his existing implant was removed by sectioning it into multiple pieces. The size of the chin and jaw angles made this necessary as they could not be slid through the much smaller and tightly scarred pocket tunnel between the two. Given this expected observation the new implant was split into two pieces and placed in a back to front direction and reunited in the middle of the chin. (In some cases the unique internal wedge design on the jaw angles may permit it to be placed as one piece)
 Custom jawline implants due to their size and extent of biologic response pose secondary placement concerns that may be different then when they were first implanted. They are easily surmountable by the experienced and expectant surgeon.
Custom jawline implants due to their size and extent of biologic response pose secondary placement concerns that may be different then when they were first implanted. They are easily surmountable by the experienced and expectant surgeon.
Case Highlights:
1) Custom jawline implants are not infrequently replaced due to patient desire to adjust the implant’s dimensions to what they now are as an improved design.
2) Custom jawline implants are associated with significant encapsulation and differing amounts of bony overgrowth at the jaw angles.
3) Depending upon implant size a previous one-piece placement may need to be replaced with a split insertion technique due to the encapsulation.
Dr. Barry Eppley
Indianapolis, Indiana