

Background: Custom facial implant designs offer a wide variety of potential facial augmentation changes. On the patient’s 3D CT scan virtually any implant design can be done. But the one important consideration that is not evident in a custom implant design is can it be surgically placed. Because of the overlying soft tissues and incisional limitations not every custom facial implant can be placed as is…meaning in one intact piece. This becomes particularly relevant when rigid implant materials are used since they have no ability to change their shape to pass through an incision.
Rigid implant materials, such as porous polyethylene (Medpor/Omnipore) and PEEK, have their merits but ease of surgical placement (and removal) are not one of them. As a result such implant materials, particularly in a long complex shape like that of a jawline, requires design and intraoperative maneuvers to get around this material liability. The obvious solution is to section the amount into pieces which will then allow them to be inserted more easily. This requires reassembly once past the incisions and inside the patient. This then introduces another variable not seen in a one piece implant…getting it to fit back together exactly as it was designed. With three pieces there is increased potential for misalignment/rotation of the pieces given the lack of visibility in surgery of where they fit together due to the soft tissues.
When such implant piece misalignment occurs the secondary challenges to correct it are increased by certain of the implant materials (porous polyethylene). The extensive tissue ingrowth makes repositioning and/or removal difficult (not impossible) and should only be attempted by those experienced in taking on these implant challenges.
Case Study: This male had a custom Medpor jawline implant placed several years previously. As is the norm for a rigid material it was designed and placed as three pieces. His surgical outcome showed that there was a misalignment to the chin piece to the back jaw pieces, a left-sided tilt, and he also desired a more square chin shape with some increased horizontal projection. The paired posterior jaw implant pieces were satisfactory in both aesthetic effect and alignment.
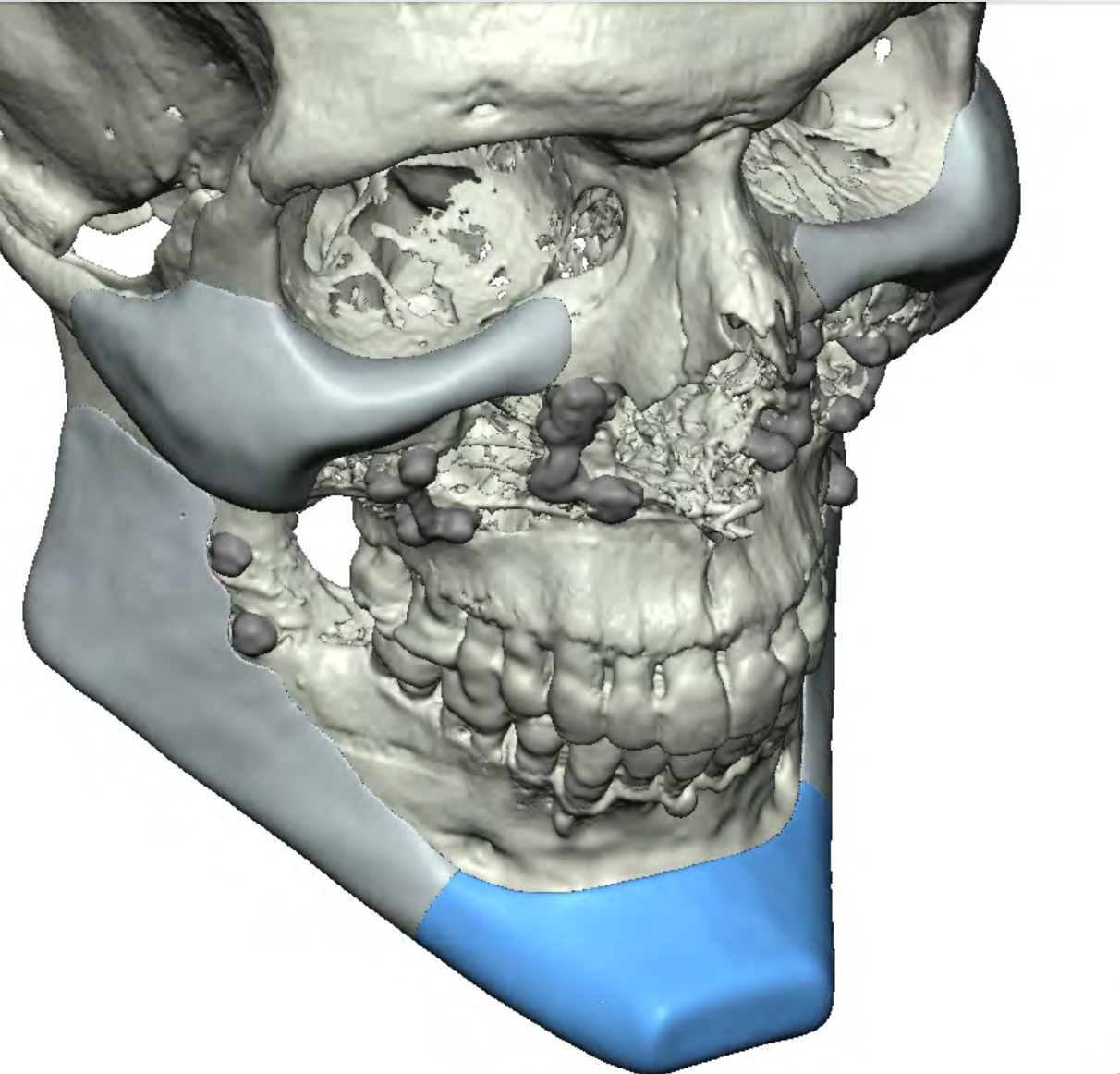
 Since Medpor can rarely be seen in a 3D CT a new chin implant piece had to be designed from the original implant design file with the presumption that they were properly (which externally felt so). The new chin implant added 5mms more horizontal projection, was more narrow (to keep in alignment with the converging lateral jaw lines) and was much more square in shape. The posterior extensions were a bit longer to ensure they contacted the back pieces and they could also be trimmed if they were too long.
Since Medpor can rarely be seen in a 3D CT a new chin implant piece had to be designed from the original implant design file with the presumption that they were properly (which externally felt so). The new chin implant added 5mms more horizontal projection, was more narrow (to keep in alignment with the converging lateral jaw lines) and was much more square in shape. The posterior extensions were a bit longer to ensure they contacted the back pieces and they could also be trimmed if they were too long.
 Under general anesthesia and through his existing submental incision the Medpor chin implant was removed in a single piece. The desired improvements in the new chin implant could be seen compared to the removed implant.
Under general anesthesia and through his existing submental incision the Medpor chin implant was removed in a single piece. The desired improvements in the new chin implant could be seen compared to the removed implant.
The anterior ends of the jaw pieces could be seen through the submental incision on both sides.

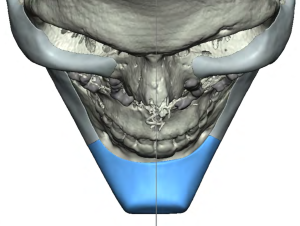
 The new Medpor chin implant was inserted and positioned in the midline and along a straight horizontal plane. The back ends of the chin implant did not require trimming and had good alignment with the posterior pieces. Double screw fixation was applied using drilled 17mm long screws.
The new Medpor chin implant was inserted and positioned in the midline and along a straight horizontal plane. The back ends of the chin implant did not require trimming and had good alignment with the posterior pieces. Double screw fixation was applied using drilled 17mm long screws.
When removing Medpor implants of any facial location the first question is always how much soft tissue trauma will it create and could it cause any permanent soft tissue injury. In this case the mental nerve was above the implant’s position so its risk of injury was low. The second question is can it be removed in its entirety and in one piece. If you can remove it in one piece that is assurance that all the material is removed whether the implant is being replaced or not.
When replacing a larger Medpor chin implant vs a slightly smaller one the intraoperative question is will it fit through the original submental incision? This one fortunately did (barely) and section it into two pieces can be done and if needed I would have done so. But keeping it intact, particularly over a solitary projecting structure like the chin, is obviously more ideal.
Key Points:
1) Part of a custom jawline implant can be re-designed and replaced if the original design is known.
2) Designing a chin implant to be more square is a function of converging jaw width lines and sharper defined chin corners.
3) Most square chin implants need double screw fixation to ensure a level horizontal axis of placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon