

Background: Facial asymmetries often have a contributing bony basis to them whether they are developmental, traumatic or pathologic in origin. One extremely unique cause of facial asymmetry is Parry-Romberg syndrome also known as craniofacial linear scleroderma. In this well known but biologically not yet understood syndrome atrophy of the facial soft tissue starts usually along the distribution of the trigeminal nerve either as a child, teenager or as an adult. The tissue loss progresses with no known way to stop it until it has burned itself out.
Once the tissue atrophy process is over the soft tissue loss can be significant but there is usually underlying bone loss as well. These tissue losses are often seen as linear indentations or having a coup de sabre (cut) appearance. The affected facial areas also have a withered or atrophic look to them.
Rconstruction of this unusual form of hemifacial atrophy initially requires the addition of soft tissue volume. Depending upon the extent of the atrophy this could be done by fat injections, dermal-fat grafts or free tissue transfers. In larger areas of involvement free tissue transfer provides a large amount of soft tissue volume which can be reshaped secondarily as is needed. The bony deformities may not always need to be treated depending upon their severity and location. But when needed custom implant designs are usually best as the bone deformity is unique in each case.
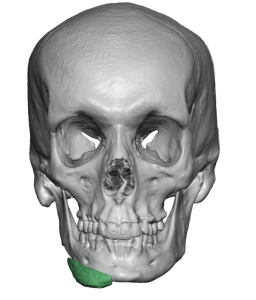
 Case Study: This male had the onset of Parry-Romberg as an adult involving his right face which was subsequently treated by a scapular free flap. This was followed by some soft tissue reductions/reshaping as well as the placement a modified chin implant along the right jawline to to try and treat the bony deficiency. His 3D CT scan showed atrophy of the right jaw and bones as well as the location of the chin implant.
Case Study: This male had the onset of Parry-Romberg as an adult involving his right face which was subsequently treated by a scapular free flap. This was followed by some soft tissue reductions/reshaping as well as the placement a modified chin implant along the right jawline to to try and treat the bony deficiency. His 3D CT scan showed atrophy of the right jaw and bones as well as the location of the chin implant.
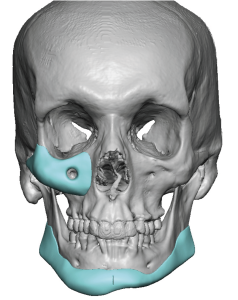
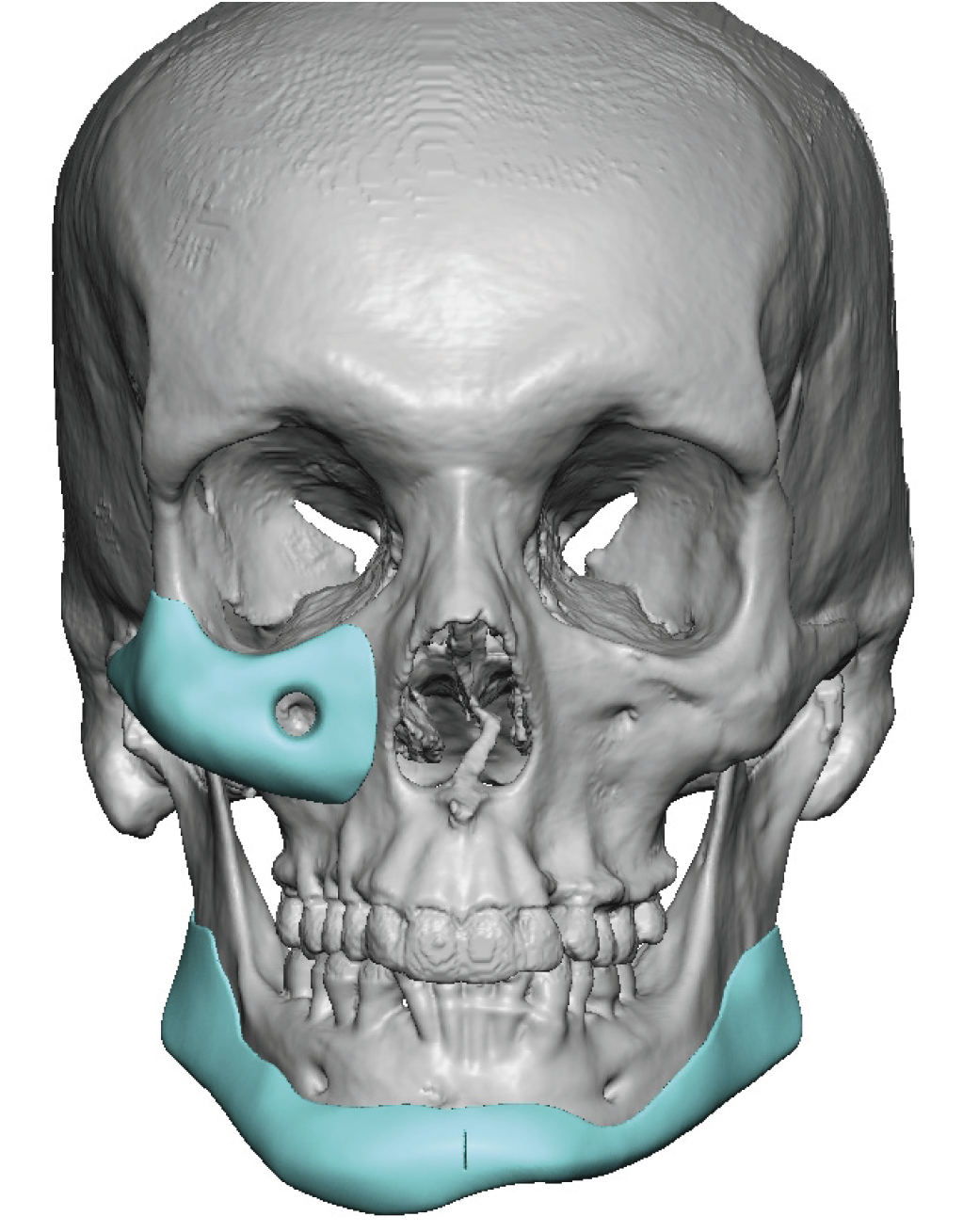
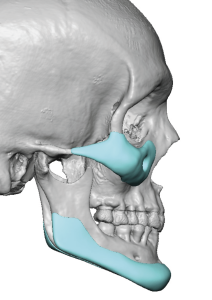 Custom implants were designed to build back the bone lost in the cheek/midface as well as along the jawline. He opted to have the left side of the jawline augmented as well creating a wrap around implant. Interestingly despite the unusual look that the chin implant seemed to create on the bone externally it had a favorable effect and thus was kept as part of the custom jawline implant design.
Custom implants were designed to build back the bone lost in the cheek/midface as well as along the jawline. He opted to have the left side of the jawline augmented as well creating a wrap around implant. Interestingly despite the unusual look that the chin implant seemed to create on the bone externally it had a favorable effect and thus was kept as part of the custom jawline implant design.
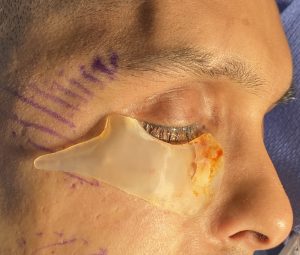
 Under general anesthesia the right midface implant was placed through an intraoral vestibular incision. The jawline implant was placed through the usual external submental and bilateral intraoral incisions. The chin implant was removed in the process.
Under general anesthesia the right midface implant was placed through an intraoral vestibular incision. The jawline implant was placed through the usual external submental and bilateral intraoral incisions. The chin implant was removed in the process.
Custom implants can play a valuable role in the reconstruction of Parry-Romberg facial atrophy. It requires adequate soft tissue thicknesses over them so their use might not be part of the primary reconstruction as this case so illustrates.
Key Points:
1) Facial asymmetry caused by Parry-Romberg are usually more severe than most developmental facial asymmetries.
2) Soft tissue reconstruction if needed should usually be done prior correction of skeletal asymmetries with implants.
3) Previously placed implants for bony asymmetry corrections provide valuable information for custom facial implant designs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon