

Background: Midface augmentation is a common aesthetic requested procedure done today by either injectable fillers or implants. But no matter how the augmentation is performed it is really a ‘spot’ technique which focuses on specific midface areas like the cheeks and undereyes which are common areas of aesthetic deficiencies. Available off the shelf implants clearly show the localized approach with cheek, paranasal-premaxillary and tear trough implants which is understandable given the market request for them.
When it comes to midface augmentation as a complete unit the concept of bone movement, specifically Lefort osteotomies, comes to mind since they provide larger areas of midface advancements. For a more total midface movement LeFort II and III osteotomies diagrammatically look effective but the magnitude of the surgery and the change in the occlusion limits their use to patients with very specific midface deficiencies.
For the aesthetic patient seeking a midface augmentation who has a satisfactory occlusion the custom midface implant offers a superior method. Not only can the specific area of surface area coverage be controlled but the thicknesses of augmentation in various areas be adjusted as needed. The biggest challenge in large surface custom midface implants is in how to surgically place it through limited incisions.
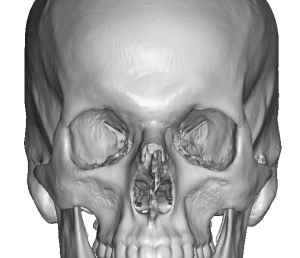
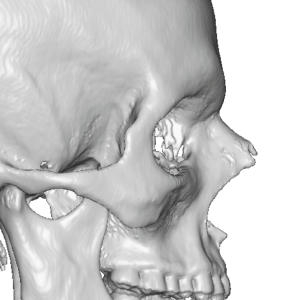 Case Study: This male had a mild midface recession that made his nose and chin projection appears more pronounced than they really were. Outwardly he identified the deficiency extending though the whole midface from the lateral brow down to the nasal base. His 3D CT supported his perception and the midface deficiency could best be seen in the periorbital area with narrowing of the lateral orbital wall and tail of the brow.
Case Study: This male had a mild midface recession that made his nose and chin projection appears more pronounced than they really were. Outwardly he identified the deficiency extending though the whole midface from the lateral brow down to the nasal base. His 3D CT supported his perception and the midface deficiency could best be seen in the periorbital area with narrowing of the lateral orbital wall and tail of the brow.
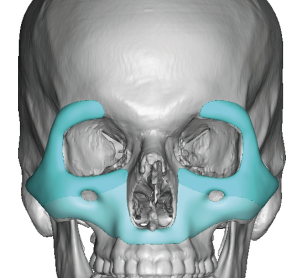
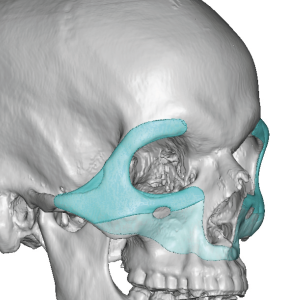
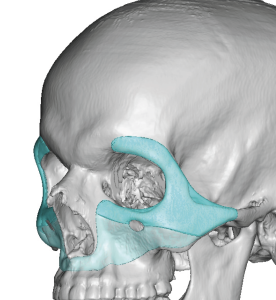
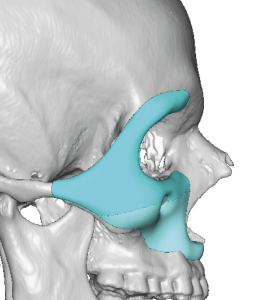 A midface implant was designed from his 3D CT scan that covered the entire midface from the lateral brow down the maxilla short of the alveolus. It was designed as three pieces that fit together along a split line at the level of the infraorbital nerve.
A midface implant was designed from his 3D CT scan that covered the entire midface from the lateral brow down the maxilla short of the alveolus. It was designed as three pieces that fit together along a split line at the level of the infraorbital nerve.
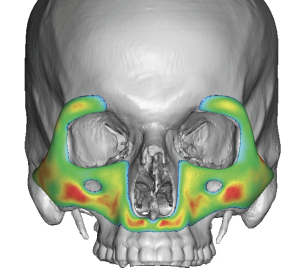 The implant’s maximal thickness was 4mms located at the maxillary concavity and paranasal areas..
The implant’s maximal thickness was 4mms located at the maxillary concavity and paranasal areas..


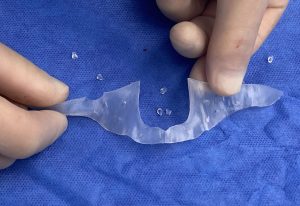
 Under general anesthesia with the implant laid out over the patient’s face raises the question was how it was going to be placed. Such a large surface area implant can be daunting for how to implant it.
Under general anesthesia with the implant laid out over the patient’s face raises the question was how it was going to be placed. Such a large surface area implant can be daunting for how to implant it.
 A three incisional approach was taken for its placement which begins with an intraoral high vestibular incision placed between the 2nd premolars. Through this access the entire midface can be degloved sparing the infraorbital nerves. The lower half of the implant was prepared by placing multiple 3mm perfusion hoes through the implant. It was then place across the lower midface from the cheeks across the nasal base from side to side and secured with single microscrew into the zygomatic buttresses. A two layer musculomucosal closure was done.
A three incisional approach was taken for its placement which begins with an intraoral high vestibular incision placed between the 2nd premolars. Through this access the entire midface can be degloved sparing the infraorbital nerves. The lower half of the implant was prepared by placing multiple 3mm perfusion hoes through the implant. It was then place across the lower midface from the cheeks across the nasal base from side to side and secured with single microscrew into the zygomatic buttresses. A two layer musculomucosal closure was done.


 For the upper half of the implants small upper and lower eyelid incision was were which permitted its passage into the implant pocket and the horizontal union with the lower half of the implant. Microscrew fixation was done at the zygoma and lateral orbital wall.
For the upper half of the implants small upper and lower eyelid incision was were which permitted its passage into the implant pocket and the horizontal union with the lower half of the implant. Microscrew fixation was done at the zygoma and lateral orbital wall.

 His intraoperative before and after showed the modest but visible total midface augmentation effect.
His intraoperative before and after showed the modest but visible total midface augmentation effect.
 The total midface implant is the only augmentation method that produce a ‘LeFort III’ effect…although these procedures are not really comparable. That only appears so on paper or in diagrams. The LeFort III osteotomy has functional benefits and changes the occlusion and nose as well. Its use is for more significant midface deficiencies. The total midface implant augments the existing bone structure and does not change the occlusion or nasal shape. (although an augmentative rhinoplasty can be done at the same time or later) Its role is for more modest midface deficiencies that have a purely aesthetic basis for doing so.
The total midface implant is the only augmentation method that produce a ‘LeFort III’ effect…although these procedures are not really comparable. That only appears so on paper or in diagrams. The LeFort III osteotomy has functional benefits and changes the occlusion and nose as well. Its use is for more significant midface deficiencies. The total midface implant augments the existing bone structure and does not change the occlusion or nasal shape. (although an augmentative rhinoplasty can be done at the same time or later) Its role is for more modest midface deficiencies that have a purely aesthetic basis for doing so.
Key Points:
1) Total midface augmentation for aesthetic purposes can only be done by a custom midface implant design.
2) The total custom midface implant must be manufactured and placed into multiple pieces to fit through intraoral and eyelid incisions.
3) This type of midface augmentation illustrates a basic custom implant concept that surface area coverage can be just as important if not more so than implant thicknesses.
Dr. Barry Eppley
World-Renowned Plastic Surgeon