

Background: Ample projection of the midface is determined by numerous bony and soft tissue landmarks. The most classic sign of a midface deficiency is an underbite. The more posterior positioning of the maxillary arch compared to the mandibular teeth can occur in isolation but often is also part of a more global midface deficiency.
In complete middle deficiency the projection of the entire midface between the forehead-brow bones and the lower jaw/chin is horizontally deficiency resulting in a flat or even concave facial profile. A Lefort I osteotomy advancement provides functional improvement but realigning the upper teeth to the lower teeth and provides increased projection to the nasal base. But the rest of the midface remains behind or unaffected above the lower maxillary osteotomy bone cut. While a LeFort III osteotomy advancement would provide a more effective and complete aesthetic effect there are some practical considerations to doing spin an adult for a primarily aesthetic effect.
The alternative approach to a LeFort III osteotomy advancement in an adult is a first stage LeFort I osteotomy with a second stage custom midface implant to complete it. The custom implant can just include what lies above the previous LeFort I or can also provide more augmentation over that area than what was achieved by the bone movement.
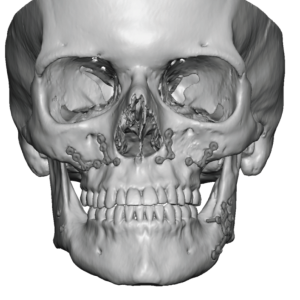
 Case Study: This female has a complete midface deficiency and had previously been through a bimaxillary procedure that included a LeFort I osteotomy advancement. While this improved her occlusion she remained flat throughout the rest of her midface. The still persistent midface flatness could be appreciated in the side view of the 3D CT scan.
Case Study: This female has a complete midface deficiency and had previously been through a bimaxillary procedure that included a LeFort I osteotomy advancement. While this improved her occlusion she remained flat throughout the rest of her midface. The still persistent midface flatness could be appreciated in the side view of the 3D CT scan.
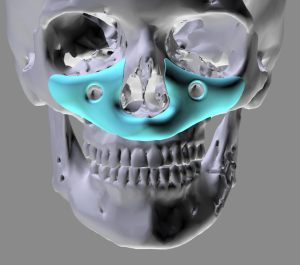
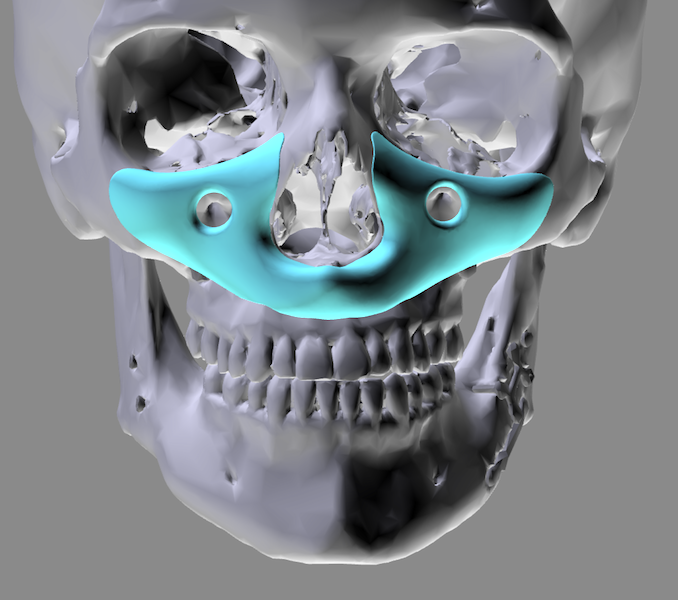
 A custom midface implant was designed to provide increased horizontal projection with the greatest thickness around and along the nasal base.
A custom midface implant was designed to provide increased horizontal projection with the greatest thickness around and along the nasal base.
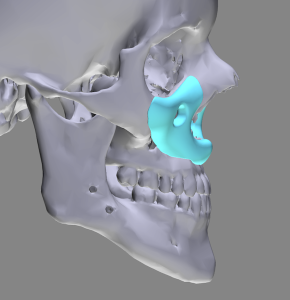
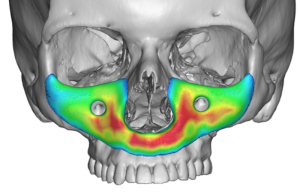 In designing a custom midface implant it is important to remember that its shape should still be concave in profile. A convex implant design in profile would produce a bump-like appearance rather than a more natural augmented shape.
In designing a custom midface implant it is important to remember that its shape should still be concave in profile. A convex implant design in profile would produce a bump-like appearance rather than a more natural augmented shape.

 Under general anesthesia her original intraoral maxillary vestibular scar was opened to deglove the entire midface with the dissection encircling the infraorbital nerve. The indwelling metal hardware provided areas of dense scar adhesion. While the hardware could be removed that may leave some open bone holes into the maxillary sinus creating the risk of postoperative contamination to the midface implant. Thus no hardware was removed.
Under general anesthesia her original intraoral maxillary vestibular scar was opened to deglove the entire midface with the dissection encircling the infraorbital nerve. The indwelling metal hardware provided areas of dense scar adhesion. While the hardware could be removed that may leave some open bone holes into the maxillary sinus creating the risk of postoperative contamination to the midface implant. Thus no hardware was removed.

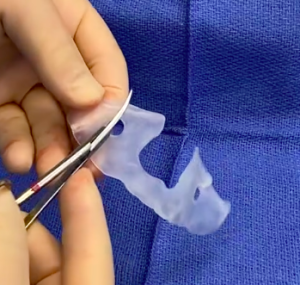
 The custom midface implant was opened and prepared for implantation by cutting a slit through the implant above the infraorbital nerve hole and placing three 4mm perfusion holes per side.
The custom midface implant was opened and prepared for implantation by cutting a slit through the implant above the infraorbital nerve hole and placing three 4mm perfusion holes per side.

 The implant was then placed, carefully checking that it encircled the infraorbital nerve and came back together above it. It was secured into position with a single screw per side. A two layer musculomucosal closure with resorbable sutures covered the implant.
The implant was then placed, carefully checking that it encircled the infraorbital nerve and came back together above it. It was secured into position with a single screw per side. A two layer musculomucosal closure with resorbable sutures covered the implant.
Total midface augmentation in an adult is hard to accomplish with a complete bony approach (LeFort III osteotomy advancement) for a variety of reasons and often is associated with numerous bony step offs and irregularities. A first stage Lefort I advancement followed by a second stage custom midface implant accomplishes the same effect with less morbidity and recovery in an adult.
Case Highlights:
1) In complete midface augmentation a LeFort I osteotomy only treats the lower dentolveolar bony segment deficiency.
2) A custom midface implant completes the facial augmentation effect not treated by a Left I advancement.
3) The custom midface implant covers the entire infraorbital-maxillary surface area leaving incorporating a relief for the infraorbital nerves.
Dr. Barry Eppley
Indianapolis, Indiana