

Background: Adequate augmentation of the deficient midface has historically been in the province of the LeFort osteotomy. While such osteotomies can be done at different levels of the midface depending on the skeletal deficiency, the one constant was the improved occlusal relationship it provided. Malocclusion was the inferior indicator and the hallmark of such midface skeletal deficiencies and also the limiting factor in how much midface augmentation resulted.
But less severe or aesthetic midface deficiencies are far more common and often exist in the presence of an orthodontically corrected occlusion. The midface deficiency is not significant enough to justify an osteotomy and the normalized occlusion is a contraindication. But the occlusal relationship aside, the magnitude of the surgery and the various bony irregularities that would result make a bony correction an unappealing and inprecise operation when viewed from an aesthetic perspective.
Historically the concept of ‘midface implants’ referred to the use of preformed cheek, tear trough or paranasal-premaxillary implant styles. While these have their merit for the spot augmentations for which they are designed, trying to patch them together to create an effective and more complete midface augmentation is fraught with aesthetic problems. The need to try and patch together standard implants to try and create a specific aesthetic effect has been replaced with the contemporary use of custom designed implants made for the patient’s specific bony anatomy.
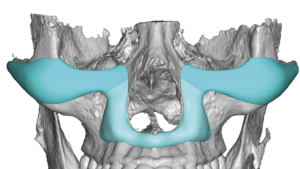
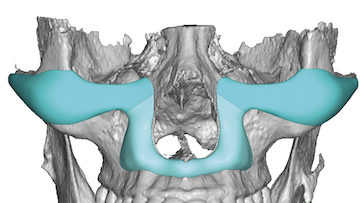
 Case Study: This male desired an augmentation to project his flatter midface forward (central projection) but not make his face significantly wider. Using a 3D CT scan implants were designed for the infraorbital rims and down and around the bony pyriform aperture area. As a paired set of implants they had the appearance of ‘angle wings’.
Case Study: This male desired an augmentation to project his flatter midface forward (central projection) but not make his face significantly wider. Using a 3D CT scan implants were designed for the infraorbital rims and down and around the bony pyriform aperture area. As a paired set of implants they had the appearance of ‘angle wings’.
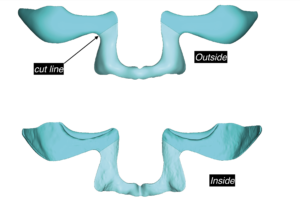 In planning for their surgical implantation, a cut line was made in the midface implants design so they could be manufactured in two pieces per side as well as placed through two different incisions. (lower eyelid and intraoral)
In planning for their surgical implantation, a cut line was made in the midface implants design so they could be manufactured in two pieces per side as well as placed through two different incisions. (lower eyelid and intraoral)


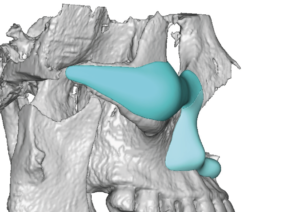
 In surgery the infraornital-malar component was placed through a lower eyelid incision and the pyriform aperture part placed through an intraoral vestibular incision. Good placement was assured by aligning them at the cut line in their design.
In surgery the infraornital-malar component was placed through a lower eyelid incision and the pyriform aperture part placed through an intraoral vestibular incision. Good placement was assured by aligning them at the cut line in their design.
Midface augmentation can now be performed using custom implant designs that target specifically the patient’s desired zones of augmentation. This is a great way to ‘pull the entire midface out’ without an osteotomy or need for change in the occlusion. Such midface implants design do very well in terms of a very low infection risk (I have not seen one yet) and being able to be accurately positioned during surgery.
Case Highlights:
1) Adding forward projection to the midface is often thought only possible with a bone movement done by some form of a LeFort osteotomy.
2) Contemporary custom midface implant designs now make it possible to selectively augment very specific areas of the midface for increased horizontal projection.
3) Custom midface implants that cover the infraorbital rims and much of the maxilla can be placed through lower eyelid and intraoral incisionns.
Dr. Barry Eppley
Indianapolis, Indiana