

Background: Pectoral implants are the seemingly male equivalent of the female breast implant. And while they are both gender-specific chest enhancement procedures that general concept is where the similarity stops. Pectoral implants have major differences from breast implants is that they are made of solid silicone, are intended to be a completely muscular enhancing implant and are limited in its placement to the transaxillary approach.
But one of the most important differences is not seen until pectoral implant revisions or pectoral implant replacements are needed. Breast implants have the advantage in that from the inframammary approach changes to the pocket in which the implant resides (capsulotomy or capsulectomies) can easily be done. But the placement of an inframammary incision in men is far less accepted for understandable aesthetic reasons. The visibility and being to work from the narrow sub pectoral tunnel from the armpit provides limited capabilities of pocket change.
Another difference becomes apparent in cases of chest asymmetry, particularly in congenital ribcage anomalies. While in breast implants breast mound asymmetries are easier to treat because the goal is a differential change in the externally visible breast mound. In essence the overlying softy tissue can be expanded by a wide variety of breast implant types, styles and sizes. But in pectoral implants there are limited implant options and understanding the differences in the shape of the ribs underneath the muscle is much harder or even impossible to fully visualize. As a result the use of standard pectoral implants in ribcage asymmetries often results in persistent symmetry and may even be greater than the natural asymmetry now being implant magnified.
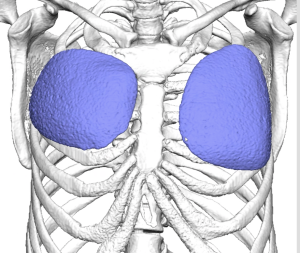 Case Study: This tall thin male presented for custom pectoral implants after having standard pectoral implants placed. The same size and style of pectoral implants were placed on both sides and what was known to be some chest asymmetry not become more apparent. There was also the aesthetic concern that the pectoral augmentation did not produce a more overall chest enhancement effect and had its greatest effect (on the normal left side) on the lower part of the muscle. His 3D CT chest scan showed the differences in the position of the existing standard pectoral implants as well as some deformity of the right ribcage under the pectoral muscle.
Case Study: This tall thin male presented for custom pectoral implants after having standard pectoral implants placed. The same size and style of pectoral implants were placed on both sides and what was known to be some chest asymmetry not become more apparent. There was also the aesthetic concern that the pectoral augmentation did not produce a more overall chest enhancement effect and had its greatest effect (on the normal left side) on the lower part of the muscle. His 3D CT chest scan showed the differences in the position of the existing standard pectoral implants as well as some deformity of the right ribcage under the pectoral muscle.
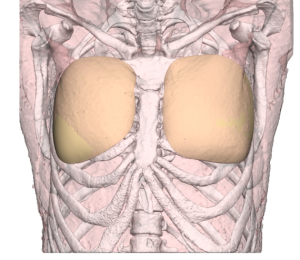 New custom pectoral implants were designed that provide a more uniform augmentation under the muscle ensuring that more volume was in the superomedial aspect of the chest compared to that of his existing implants.
New custom pectoral implants were designed that provide a more uniform augmentation under the muscle ensuring that more volume was in the superomedial aspect of the chest compared to that of his existing implants.

 Under general anesthesia and through his existing healed axillary incisions the standard pectoral implants were removed and compared to the new custom ones.
Under general anesthesia and through his existing healed axillary incisions the standard pectoral implants were removed and compared to the new custom ones.
On the inner surface of the new custom pectoral implants the negative impression of the underlying ribs could be seen. In theory this may help it fit better onto the ribcage.

 The constricted pocket on the asymmetric right side was released/ecpanded by elevators without any undue bleeding. The new implants were inserted using a funnel technique and the incisions closed. The differences on the operative table were evident.
The constricted pocket on the asymmetric right side was released/ecpanded by elevators without any undue bleeding. The new implants were inserted using a funnel technique and the incisions closed. The differences on the operative table were evident.

 When seen the next day in the upright position the improvement in the chest asymmetry was more apparent.
When seen the next day in the upright position the improvement in the chest asymmetry was more apparent.
Knowing when to opt for a custom pectoral implant approach is not widely appreciated. But in my experience the one absolute indication is when standard implants have not worked well in the face of bony ribcage asymmetries. And I would take that approach with chest wall asymmetries even before any implants are placed. These are just hard problems to optimally correct by eyeballing it in surgery. And within today’s 3D CT scanning there really is no reason to do so.
Key Points:
1) Pectoral augmentation in congenital ribcage asymmetries with standard implants is prone to perpetuating or magnifying the asymmetry.
2) A 3D CT scan of the chest/ribcage is the most accurate method to determine the exact bony differences between the sides of the chest and the standard implants they may contain.
3) In pectoral implant revisions/replacements the ability to adjust the existing pocket/capsule is more limited than in female breast implants.
Dr. Barry Eppley
World-Renowned Plastic Surgeon