


Background: Buttock implants are placed through a mid-gluteal crease incision and into either an intramuscular, submuscular or subcutaneous tissue pocket. By virtue of its placement location and the incision needed to perform it implants augment the upper 2/3 s of the buttocks in most cases. Contrary to popular perception they do not create an overall buttock enlargement that is augments the lower pole as much as it does the upper pole. This is why loose buttock tissues on its lower pole will not expand or fill out with any form of a traditional buttock implant technique.
But when lower buttock augmentation is where the only focus of the volume is needed, which is rare, a different approach is needed. This is below where an implant can be placed in any intra- or submuscular pocket and a long way to get there for a subcutaneous approach from a midline gluteal cleft incision. An infragluteal crease incision is needed for direct access to develop the pocket.
While the infragluteal crease incision is an unusual approach for placing buttock implants the pocket in which it must rest is also uncommon. At the inferior edge of the gluteus maximus muscle the sciatic nerve is not that far below it. Thus the implant must stay above the muscle. Being on the lower side of the buttocks where one has to sit on the implant with the incision close to it in a relatively thin soft tissue cover additional strategies are needed to prevent the risks of incisions dehiscence and implant exposure.
 Case Study: This 72 year-old female presented with a very unusual buttock deformity. The lower third of her buttocks was volume deficient with a large concavity/indentation.
Case Study: This 72 year-old female presented with a very unusual buttock deformity. The lower third of her buttocks was volume deficient with a large concavity/indentation.

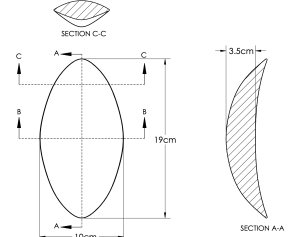 Measurements were made of the lower buttock indentations including its depth which had a V-shape down along its longitudinal axis. From these measurements a computer design drawing was made from which the implants were manufactured.
Measurements were made of the lower buttock indentations including its depth which had a V-shape down along its longitudinal axis. From these measurements a computer design drawing was made from which the implants were manufactured.

 To help with tissue adherence ePTFE strips were placed onto the buttock implant underside.
To help with tissue adherence ePTFE strips were placed onto the buttock implant underside.

 Under general anesthesia and in the prone position infragluteal incisions were made on each side. Pockets were developed on top of the gluteal fascia and extended beyond the muscle at the implant’s superior portion.The implants were inserted and checked for tension free closure.
Under general anesthesia and in the prone position infragluteal incisions were made on each side. Pockets were developed on top of the gluteal fascia and extended beyond the muscle at the implant’s superior portion.The implants were inserted and checked for tension free closure.
 Then Galaflex mesh applied over them and sewn down around the implant. Drains were placed prior to incisional closure
Then Galaflex mesh applied over them and sewn down around the implant. Drains were placed prior to incisional closure
 When seen two weeks later for drain removal the implants had made good improvement albeit not ideal. More implant volume would have been even more beneficial but a major improvement for sure.
When seen two weeks later for drain removal the implants had made good improvement albeit not ideal. More implant volume would have been even more beneficial but a major improvement for sure.
 The incisional tapes were removed and her early scar results were encouraging.
The incisional tapes were removed and her early scar results were encouraging.
This case of buttock implant augmentation poses numerous unique challenges. The first is the problem itself as. such lower buttock indentations are rare and how to treat them unprecedented. Usually fat injections would be the typical approach but in a 72 year old with not significant fat to harvest this was not an option. Placing implants through an infragluteal incision into a more superficial tissue pocket has risks that traditional buttock implants do not have. The pressure of sitting on the implants raises short term concerns about incisional security which is paramount with an implant not too far away.
Key Points:
1) Traditional buttock implants when placed intra- or submuscular augment the middle and upper portions of the buttocks and not the lower pole.
2) In this unique case of lower buttock volume loss/indentations an infragluteal approach to buttock implant placement was done on top of the gluteus maximus muscle fascia.
3) A moulage custom implant fabrication process was done to create the unique shape of the buttock implants needed.
4) To encourage implant stability /fixation in a lower buttock implant pocket above the muscle the combination of ePTFE strips were manufactured onto the implant as well as Galfaflex mesh placed over the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon