

Background: Hip contouring historically was a reductive procedure for which liposuction was the definitive treatment. While that aesthetic body contouring need still exists today the reverse, hip augmentation, has become a commonly requested procedure. Driven by the increasing demand for buttock augmentation as well as male to female gender affirming surgeries the role of hip augmentation in body contouring generates great interest.
While synthetic fillers have a role in hip augmentation around the world, their use in the U.S. is far more limited due to lack of an FDA-approved filler to do so. Off the shelf injectable fillers, such as Sculptra, are used but the cost is significant and the result limited given the volume off filler needed. This leaves fat injections as the most common hip augmentation procedure done, often in combination with BBL surgery. The lack of sustained volume retention with hip fat injections particularly in the trochanteric region, usually the deepest of a hip contour deformity, is well known This hip area, known as the hip dips, is the most adherent region and usually has the least amount of subcutaneous fat over the trochanteric head of the femur.
While implants are always an option in hip augmentation surgery they have their own unique set of problems given the anatomic location in which they have to be placed. Thus I always advise patients to try fat injections first to see how much result they can get and save hip implants as a last resort. In rare cases run which a tummy tuck is being performed there is a unique fat grafting technique available.

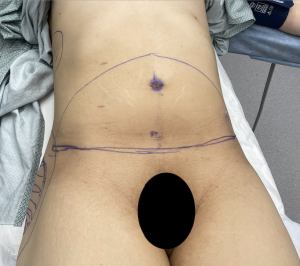
 Case Study: This female was to undergo a combined body contouring procedure of shoulder reduction and a tummy tuck. Even though she was young she had lost over 50lbs of body weight and ended up with a lower abdominal pooch. She also had hip dips with an otherwise lack of a visible hip convexity in frontal profile. We discussed doing fat injections for the hips by suctioning the abdomen first and then doing the tummy tuck or taking the tissue discard from the tummy tuck and using it as large composite (dermal-fat) grafts placed directly into the hip dips through the ends of the tummy tuck. She chose the dermal-fat graft implantation approach.
Case Study: This female was to undergo a combined body contouring procedure of shoulder reduction and a tummy tuck. Even though she was young she had lost over 50lbs of body weight and ended up with a lower abdominal pooch. She also had hip dips with an otherwise lack of a visible hip convexity in frontal profile. We discussed doing fat injections for the hips by suctioning the abdomen first and then doing the tummy tuck or taking the tissue discard from the tummy tuck and using it as large composite (dermal-fat) grafts placed directly into the hip dips through the ends of the tummy tuck. She chose the dermal-fat graft implantation approach.

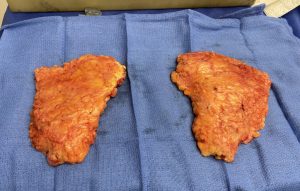 Under general anesthesia and in the supine position the lower abdominal tissue were excised in a supraumbilical technique and cut into two pieces. The overlying skin was removed in preparation for implantation.
Under general anesthesia and in the supine position the lower abdominal tissue were excised in a supraumbilical technique and cut into two pieces. The overlying skin was removed in preparation for implantation.



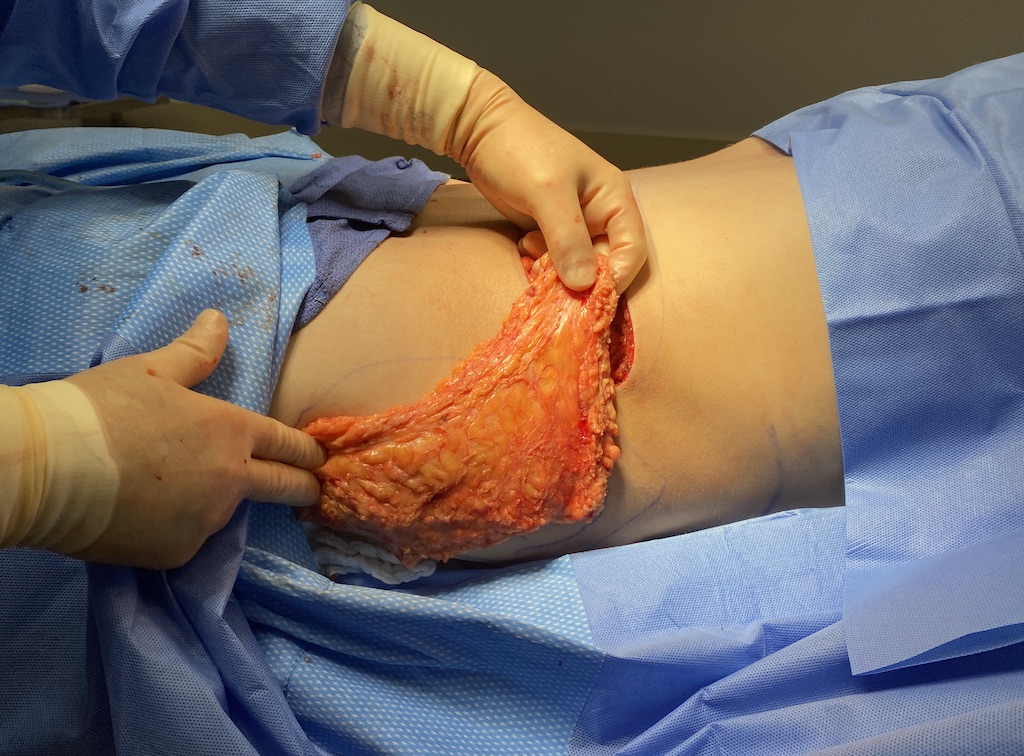
 Through the ends of the open tummy tuck pockets were dissected out over the hip dip areas at the deep subcutaneous level. The fat grafts were passed into the pocket by a percutaneous suture technique which was secured to the overlying skin by a bolster.
Through the ends of the open tummy tuck pockets were dissected out over the hip dip areas at the deep subcutaneous level. The fat grafts were passed into the pocket by a percutaneous suture technique which was secured to the overlying skin by a bolster.
The upper portion of the graft was suture to the fascia at the outer end of the tummy tuck. Thus the fat graft was stretch out over the length of the pocket so it was smooth which also gave it the best chance of survival through rapid revascularization from the surrounding tissues. The tummy tuck was then closed with umbilical transposition.
 Her intraoperative before and after pictures show the body contouring changes with abdominal flattening and hip augmentation.
Her intraoperative before and after pictures show the body contouring changes with abdominal flattening and hip augmentation.
Dermal-fat grafting is a well known technique in facial surgery although it has been over shadowed and largely forgotten with the emergence of fat injection techniques. The concept of dermal fat grafting is that a solid piece of fat can survive when implanted due to rapid reconnection of the existing blood vessels in the graft with the surrounding tissues. In smaller dermal-fat grafts in the face this has proven to be effective but they are of much smaller size. In larger dermal-fat grafts in the body, however, how well this older fat grafting method will work is less assured due to the larger size grafts needed. And there would usually be no need to do so because of the more versatile technique of fat injection grafting.
But in the face of poor volume retention with fat injection grafting into the hips and the need for a tummy tuck this raises the possibility of using a dermal-fat grafting hip augmentation method. While such larger dermal-fat grafts in the body have more risk of failing to survive there are several intraop and postoperative maneuvers that need to be done to improve its chances for survival. Making the grafting is completely laying flat and extended is done intraoperatively by various suture techniques. Postoperatively good compression over the hips by garments keeps it laying flat and ensures good contact with the surrounding tissues.
It is unknown how well these large dermal-fat grafts will work for hip augmentation. But given the need for a tummy tuck and having such tissue available at no harvest cost (need for a separate harvest site) makes their use possible. At worst much of the graft resorbs but any graft retention will be better than what fat injections could achieve. At best the hip dips are eliminated and the patient could either leave that accomplishment alone or secondarily add implants where the additional fat layer may help mitigate some of their known problems.
Case Highlights:
1) Hip augmentation remaions a challenging surgical body contouring procedure as both fat injections and hip implants have their issues.
2) A tummy tuck presents a unique opportunity for fat grafting given the large tissue discard that is available.
3) Large dermal-fat grafts taken from the tummy tuck can be used for subcutaneous augmentation of the trochanteric depression of the hips.
Dr. Barry Eppley
Indianapolis, Indiana