

Background: In many aspects the shape of the buttocks is similar to that of the breasts. They are both soft tissue mounds that sit on the side the body with a muscular base. Both can have different mound sizes from to small to large that are subject to the effects of gravity and weight loss and can be augmented with injectable fat grafting and implants. They also share tissue folds that define their inferior extent and have a major role to play in the symmetry between their two sides. Both the infragluteal and inframammary folds are also prone to undesired lowering (ptosis) which elongates their shape.
Unlike the inframammary fold in the breasts, however, the buttock infragluteal fold is subject to repetitive sitting and bending over. This can have the effect of naturally altering the stability of the fold’s position. This can be one source of infraglueal fold asymmetry where one fold is lower than the other. (which can also just be natural development as well) In such asymmetry one infraguteal fold can be lower while the one side is at a normal level or both sides can be lowered than desired with one worse than the other.
The treatment of infragluteal fold asymmetry consists only two corrective types of treatement. The most commonly done is liposuction where tissue is aspirated above the lowered fold in an attempt to get it to stick down to create a higher fold level. While this may be effective in some cases, I have never seen it to be so and it usually just causes another problem… which is loose skin above the lower infragluteal fold. The other and more definitive approach is as lower buttock lift or tuck which removes lower buttock tissue and recreates the fold at a higher level.
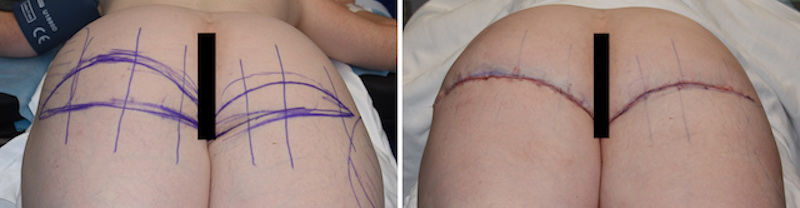
 Case Study: This female has previously been through fat injection buttock augmentation with some residual contour asymmetries. But she was most bothered by a persistent infragluteal fold asymmetry and the desire to raise the fold level even on the side of the higher infragluteal fold. She wanted the most definitive approach of lower buttock lifts. Before surgery in the standing position, a larger crescent-shaped tissue excision was marked on the lower side. Small areas of liposuction were marked to improve buttock and thigh contour concerns.
Case Study: This female has previously been through fat injection buttock augmentation with some residual contour asymmetries. But she was most bothered by a persistent infragluteal fold asymmetry and the desire to raise the fold level even on the side of the higher infragluteal fold. She wanted the most definitive approach of lower buttock lifts. Before surgery in the standing position, a larger crescent-shaped tissue excision was marked on the lower side. Small areas of liposuction were marked to improve buttock and thigh contour concerns.


 Under general anesthesia and in the prone position (with her hips flexed at 45 degrees), the wedges of skin and fat were removed as marked down to the gluteal fascia at the apex of the wedges. Closure was done using multiple dermal-fascial-dermal sutures prior to dermal-dermal and subcuticular skin closures. After the closure the elevated and improved position of the infraglutealfolds could be seen. Layered taping was applied as a dressing.
Under general anesthesia and in the prone position (with her hips flexed at 45 degrees), the wedges of skin and fat were removed as marked down to the gluteal fascia at the apex of the wedges. Closure was done using multiple dermal-fascial-dermal sutures prior to dermal-dermal and subcuticular skin closures. After the closure the elevated and improved position of the infraglutealfolds could be seen. Layered taping was applied as a dressing.
The definitive elevation and re-creation of the infragluteal folds is tissue excision. Differential infragluteal fold elevation can be done by altering the width and length of the tissue excisions. It is very difficult, and perhaps not really possible, to elevate a ptotic infragluteal fold by liposuction. This is not known to work in the breast and is never even presented as a viable treatment option for it. There would be no reason to suspect that it would work any better in the buttocks.
Case Highlights:
1) The infragluteal fold is a defining anatomic landmarks that plays a major role in the perception of buttock asymmetry.
2) A lower infragluteal fold is a frequent source of buttock asymmetry even in the presence of bilateral lower buttock ptosis.
3) Differential lower buttock lifts is the surgical procedure for asymmetric infragluteal fold levels….not liposuction.
Dr. Barry Eppley
Indianapolis, Indiana