


Background: The projection of the central midface, excluding that of the nose, is controlled by the development of the maxillary bone around the large nasal cavity. This is known as the bony pyriform rim not which the external nose, particularly that of the nostrils laterally and the columella centrally sit. It is divided into a central premaxillary region and a lateral paranasal region. Anatomically the premaxillary region is controlled by the anterior nasal spine of the maxilla and its amount of projection. The paranasal region is larger with an L-shape (right side) or reverse L-shape (left side) as it wraps around the nasal cavity. The actual rim is a to raised by the bone right next to it is concave like the rest of the maxilla.
While there is some overlap between the premaxillary and the paranasal regions they are often thought of as distinctly different based on the implants designed to augment them. Historically the lone preformed implant available to augment this central midface region was the silicone Peripyriform implant. This was a combined premaxillary and paranasal implant that wrapped around the entire pyriform aperture as the name suggests. But today’s central midface implants have evolved with different types of material compositions and implant designs.
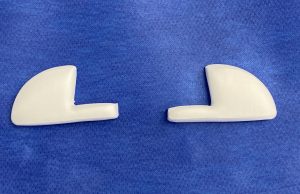 ePTFE implants provide the most contemporary approach to permanent nasal base augmentation and are available in both premaxillary and paranasal implant styles. Made from expanded polytetrafluoroethylene (ePTFE) material, the paranasal implant design includes a medial horizontal small arm connected to an outer larger vertically oriented nasal base. The implant is designed to fit snug up underneath the nostrils. With this implant design projection is achieved to push the nostrils/nasal base forward but without crossing the premaxilary/anterior nasal spine area. Given its location it can also help decrease the depth of the nasolabial folds by the side of the nose.
ePTFE implants provide the most contemporary approach to permanent nasal base augmentation and are available in both premaxillary and paranasal implant styles. Made from expanded polytetrafluoroethylene (ePTFE) material, the paranasal implant design includes a medial horizontal small arm connected to an outer larger vertically oriented nasal base. The implant is designed to fit snug up underneath the nostrils. With this implant design projection is achieved to push the nostrils/nasal base forward but without crossing the premaxilary/anterior nasal spine area. Given its location it can also help decrease the depth of the nasolabial folds by the side of the nose.
 Case Study: This male had a flatter central midface with deeper nasolabial folds. He desired to have some increased projection of the base of the nose but without any change in his nasolabial angle. 6mm ePTFE paranasal implants were chosen for the augmentation.
Case Study: This male had a flatter central midface with deeper nasolabial folds. He desired to have some increased projection of the base of the nose but without any change in his nasolabial angle. 6mm ePTFE paranasal implants were chosen for the augmentation.
 Under general anesthesia and through bilateral 1cm high vestibular incisions under the base of the nose subperiosteal pockets were dissected out along the base of the nose. Care was taken to not inadvertently penetrate the nasa mucosa.
Under general anesthesia and through bilateral 1cm high vestibular incisions under the base of the nose subperiosteal pockets were dissected out along the base of the nose. Care was taken to not inadvertently penetrate the nasa mucosa.
 Due to the L-shape of the implant the incision did not need to be as big as the implant. The inside pocket needed to be able to have the implant lay flat once inside. But the implant could be inserted through a small entrance incision by using the implant’s shape to navigate it through a much smaller incision than the implant’s size would suggest possible. Closure was done with a few resorbable sutures.
Due to the L-shape of the implant the incision did not need to be as big as the implant. The inside pocket needed to be able to have the implant lay flat once inside. But the implant could be inserted through a small entrance incision by using the implant’s shape to navigate it through a much smaller incision than the implant’s size would suggest possible. Closure was done with a few resorbable sutures.

 When seen one year later he had a visible augmentation effect with no palpable edges of the implant.
When seen one year later he had a visible augmentation effect with no palpable edges of the implant.
Augmentation of the lateral nasal base requires an implant that wears around the pyriform aperture and has a tapered edge out into the canine fossa of the maxilla. Since the canine fossa of the maxilla has a very deep concavity to it it is important that the paranasal implant has a very tapered edge laterally or an external bump will felt lateral to the side of the nostril.
Case Highlights:
1) Standard square style chin implants primarily rely on rounded width for its effect which is not particularly effective.
2) In making a more square chin, either as a custom chin or around jawline implant, the key design element is angular chin corners and a more narrow chin width.
3) Standard chin implants, even with good results, often serve as a springboard into a more complete jawline augmentation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon