

Background: Chin implants, like all implants placed in the body, induces a biologic response at the implantation site. The most well known response is encapsulation or the surrounding of the implant with scar tissue known as the capsule. Regardless of the implant material capsules are formed. Chin implants have also been associated with ‘erosion’ although this is an inaccurate biologic term for what is occasionally seen. The proper biologic response is imprinting, a passive settling into the bone that is self-limiting. It occurs as a result of pressure release or adaptation to a foreign material that expands the natural biologic boundaries of the implantation site. Interestingly it is not always seen and the size of the chin implant does moot seem to correlate to its occurrence.
An overlooked but equally occurring response to a chin implant is bone overgrowth, a reaction that is seen just as often if not more so than imprinting. A thin layer of bone is seen that has grown along the sides of the implant and occasionally completing encasing it. This is clearly a reaction to the elevation of the periosteum of the bone to create the implant pocket. But it is also reflective of a reparative response to the presence of the implant as its tries to heal over it, indicating that the implant is not causing inflammation by its presence.
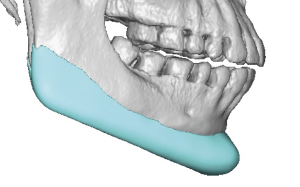
A fair number of custom jawline implant patients have a prior history of a chin implant. Some are desiring to expand the chin implant footprint or are unhappy with the chin implant result, they desire to graduate to a complete jaw augmentation effect. The need for a 3D CT scan to design the jawline implant creates an opportunity to see the chin implant as well as the localized reaction to it. The presence and amount of bone overgrowth can be seen and the need for its removal anticipated.
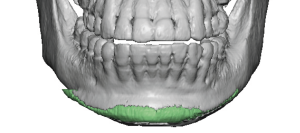
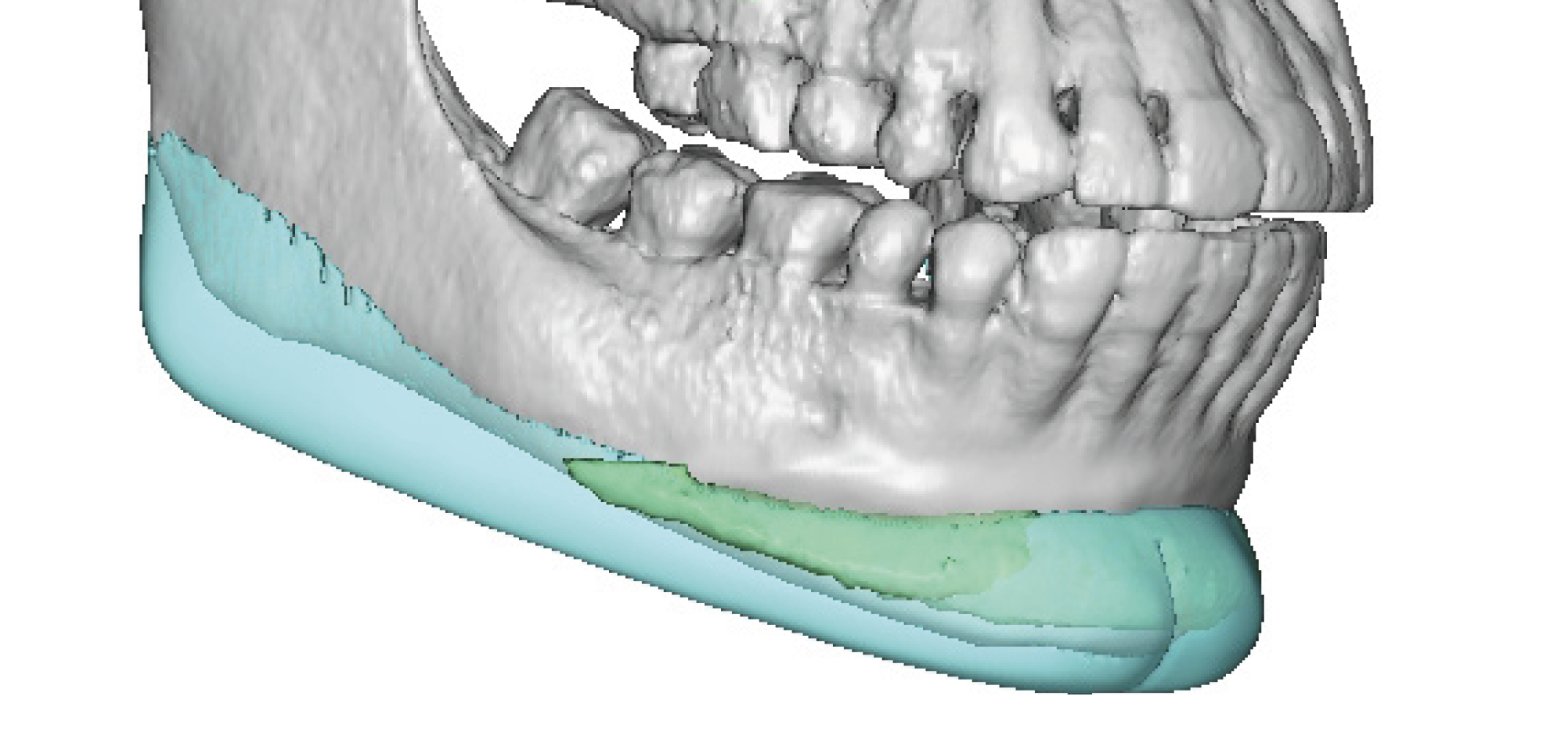
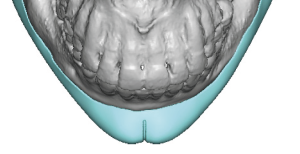
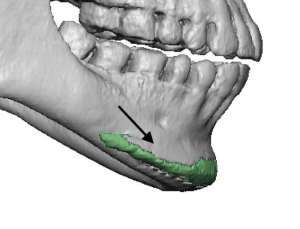
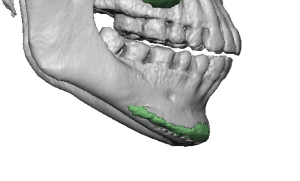 Case Study: This female had a small 4mm extended anatomic chin implant placed years before but wanted a complete jaw augmentation effect with a cleft chin. The 3D CT scan showed a large amount of bone overgrowth onto the implant particularly along the upper half of the implant. There was bone overgrowth along the bottom edge but not as significant.
Case Study: This female had a small 4mm extended anatomic chin implant placed years before but wanted a complete jaw augmentation effect with a cleft chin. The 3D CT scan showed a large amount of bone overgrowth onto the implant particularly along the upper half of the implant. There was bone overgrowth along the bottom edge but not as significant.
 A custom jawline implant was designed that was suited for a female to create a v line shape effect. The chin cleft part was a personal choice and is not typically associated with female jawline implants.
A custom jawline implant was designed that was suited for a female to create a v line shape effect. The chin cleft part was a personal choice and is not typically associated with female jawline implants.
 This translates to a vertical lengthening jawline design with minimal width and a narrow more V-shaped chin.
This translates to a vertical lengthening jawline design with minimal width and a narrow more V-shaped chin.

 Under general anesthesia and through her existing submental incision scar the chin implant was exposed. After its removal the bony overgrowth was fully exposed and removed in pieces with an osteotome.
Under general anesthesia and through her existing submental incision scar the chin implant was exposed. After its removal the bony overgrowth was fully exposed and removed in pieces with an osteotome.

 The jawline implant was inserted through the submental incision and the angle part aided into position by small posterior vestibular incisions. The chin cleft was made deeper in the midline through which a drilled long screw was placed for fixation.
The jawline implant was inserted through the submental incision and the angle part aided into position by small posterior vestibular incisions. The chin cleft was made deeper in the midline through which a drilled long screw was placed for fixation.
 Chin implants can be associated with varying amounts of bine overgrowth. While it is necessary to remove the bone overgrowths so the new custom jawline implant can have a fit as it was designed, not all of the bone needs to be removed. Maintaining the bony overgrowth under the mental nerve can help protect it from a stretch injury with the passage of the jawline implant underneath it.
Chin implants can be associated with varying amounts of bine overgrowth. While it is necessary to remove the bone overgrowths so the new custom jawline implant can have a fit as it was designed, not all of the bone needs to be removed. Maintaining the bony overgrowth under the mental nerve can help protect it from a stretch injury with the passage of the jawline implant underneath it.
Key Points:
1) Chin implants are often associated with a bone reparative response as seen by areas of bone overgrowth.
2) In replacing chin implants with a custom jawline implant it is often necessary to remove the bone overgrowths for the custom jawline implant to fit properly.
3) Such chin implants overgrowths can be seen on the custom implant 3D scan so the location and extent of bone removal is known beforehand.
4) Preserving the roof of the bone overgrowth around the mental nerves helps protect them during the placement of the custom jawline implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon