

Background: V line surgery has become popular over the past decade for those seeking a slimmer lower face. It has its origins in Asia where fuller and wider lower jaws are more common, particularly in women. It is a procedure that is done by a combination of an oblique line of jaw angle and body vertical bone resection (amputation) combined with a t-shaped chin reshaping procedure.
While V line surgery is very effective it has several specific aesthetic tradeoffs in some patients. The most common is soft tissue sagging due to the loss of structural support. This can be seen at the jaw angles with the development of jowling and at the chin with soft tissue chin pad ptosis.
But an often unspoken and less recognized aesthetic effect is that of surgical regret. Some patients can never adapt psychologically to their new facial shape. They don’t recognize themselves, their family and friends may not view the facial change kindly, or they determine they like their original facial shape better. (which is not rare in any form of facial structural surgery) The aggressive nature of the amputation of the jaw angle, creating a steep and unnatural mandibular plane angle, is usually the culprit in my observation. The very maneuver that makes it effective for significant lower facial narrowing is also what can be too extreme for some patients.

 Case Study: This female had a combined bimaxillary orthognathic surgery procedure with V line surgery in Korea. She could never adapt to her new look and wished it to be completely reversed. She did not have a 3D CT scan of her face before the surgery. A current 3D CT scan showed her indwelling hardware as well as the cut line from the V line surgery and at the osteotomy lines of the chin.
Case Study: This female had a combined bimaxillary orthognathic surgery procedure with V line surgery in Korea. She could never adapt to her new look and wished it to be completely reversed. She did not have a 3D CT scan of her face before the surgery. A current 3D CT scan showed her indwelling hardware as well as the cut line from the V line surgery and at the osteotomy lines of the chin.
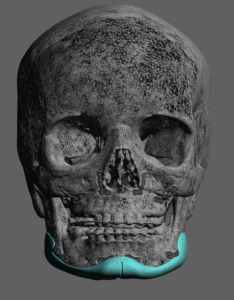
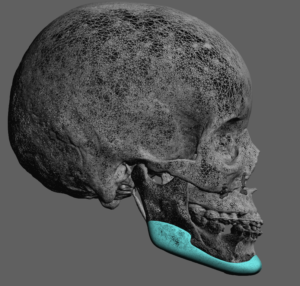
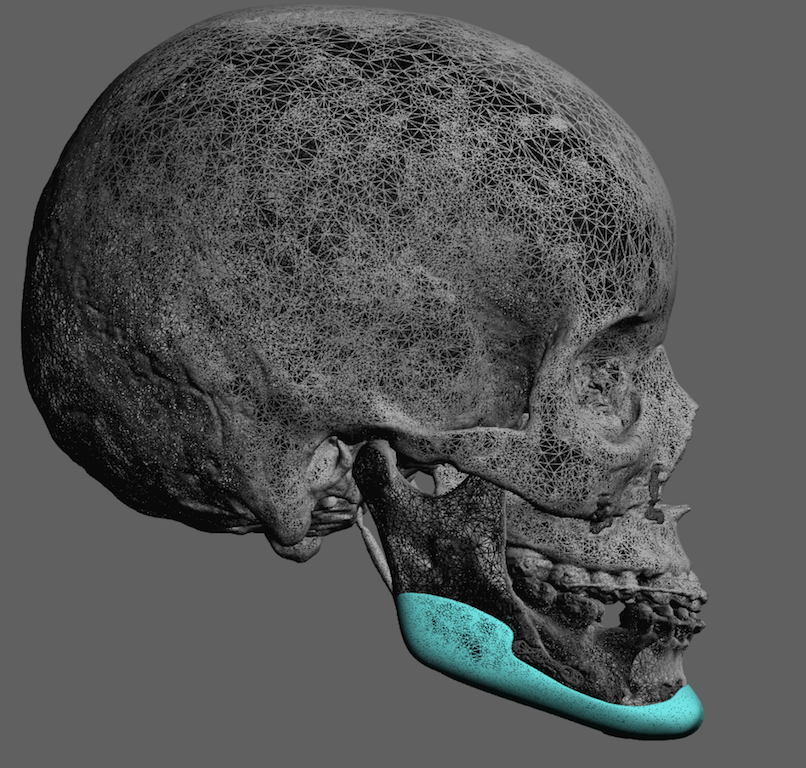
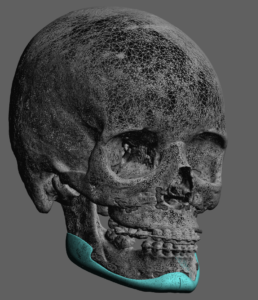 Using her 3D CT scan a jawline implant was designed that was believed to restore her jawline shape. The only reference was her before and after lateral cephalometric x-rays. Her total implant volume was 9.5ccs.
Using her 3D CT scan a jawline implant was designed that was believed to restore her jawline shape. The only reference was her before and after lateral cephalometric x-rays. Her total implant volume was 9.5ccs.


 Under general anesthesia and through a 2 cm submental incision the scarred tissues were released along all the inferolateral borders of the chin and back to the jaw angles. The jaw angle dissection was completed using intraoral incisions as getting the stuck tissues off of the hardware was important for proper implant positioning. Once the implant was inserted and positioned single screw fixation was used for the chin and double screw fixation for the jaw angles.
Under general anesthesia and through a 2 cm submental incision the scarred tissues were released along all the inferolateral borders of the chin and back to the jaw angles. The jaw angle dissection was completed using intraoral incisions as getting the stuck tissues off of the hardware was important for proper implant positioning. Once the implant was inserted and positioned single screw fixation was used for the chin and double screw fixation for the jaw angles.
V line surgery in its traditional form removes much of the inferior border of the jawline. In restoring part or all of what was removed defies any off the shelf implant/implant material. Recreating the inferior border bony contour of the lower jaw can only be done by a custom implant design approach. What the restored shape and volume restoration should be ideally obtained by having a preoperative 3D CT prior to the V line surgery. But this is very uncommon. It is more common that before and after lateral cephalometric x-rays are available from which a reasonable implant she estimation can be made.
Case Highlights:
1) The aggressive nature of V line surgery can give some patients postoperative regret who then wish to partially or fully restore their jawline shape.
2) Only a custom jawline implant concept can augment the entire inferior border of the jawline as well as add width if needed.
3) While it is ideal to have original preoperative x-rays to know what the lower jaw shape was, it is not an absolute requirement for the implant design.
Dr. Barry Eppley
Indianapolis, Indiana