

Background: Rhinoplasty surgery has been around for almost a hundred years and has its recent origin from European surgeons who attempted to reduce the large ethnic humps on the bridge of the nose. While rhinoplasty surgery has evolved tremendously and now focuses on a more complete approach to rhinoplasty, hump reduction is still a major driving reason patients seek rhinoplasty and is often part of many major nose reshaping efforts today.
Nasal hump reduction lies in the upper half of the nose and is seemingly simple. It is often taken for granted that it is the most uncomplicated rhinoplasty manuever which is an inaccurate perception. A nasal hump occurs at the junction of the nasal bones and upper lateral cartilages and septum and is rarely effectively reduced by simple rasping. (which only works on bone) It requires reduction of both bone and cartilage which is initially done by separating the upper lateral cartilages from the septum. From there the cartilage hump is reduced by taking down the high septum. This then allows the bony portion of the hump to be taken by either osteotomes or rasps.
Taking down the hump will often create the so called “open roof” deformity which is closed by reshaping the sides of the nasal bones by creating fracture lines with small osteotomes. This allows the nasal bones to fall inward, closing the open roof. Most of these osteotomies are never completely visualized even in the most open rhinoplasty. But closure of the open roof is not the end of the hump reduction, final smoothing of the nasal bones is needed as well as re-establishing the septal-upper lateral cartilage relationship which may include the use of spreader grafts.
Case Study: This 26 year-old female wanted to improve the shape of her nose. She always wanted to reduce the hump on her nose. But she not only wanted it reduced, she wanted more of a swoop or concavity to the bridge of the nose. She had good tip projection and rotation as judged by the nasolabial angle. Her tip only needed some width narrowing but no other changes.
 Under general anesthesia, an open rhinoplasty was performed with hump reduction as previously described. After closing the open roof, the upper lateral cartilages were put back to the reduced septum height and auto spreader grafts done by folding the redundant upper lateral cartilages over on themselves. Tip shaping sutures were placed but no cartilage was removed from the cephalic margins.
Under general anesthesia, an open rhinoplasty was performed with hump reduction as previously described. After closing the open roof, the upper lateral cartilages were put back to the reduced septum height and auto spreader grafts done by folding the redundant upper lateral cartilages over on themselves. Tip shaping sutures were placed but no cartilage was removed from the cephalic margins.
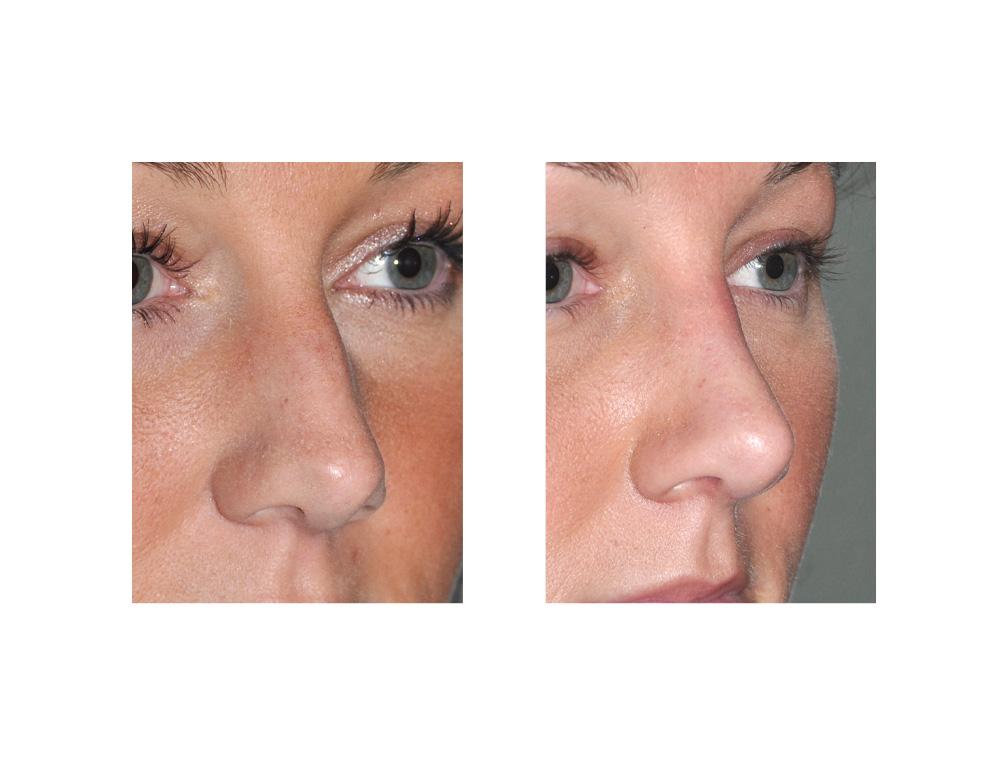 As her results show, a near isolated hump reduction rhinoplasty can be done if other structures of the nose need no to minimal manipulation. For most patients this is not possible since significant hump reduction usually changes how the tip of the nose looks as well as the overall nasal length. Computer imaging will make this need clear before surgery. isolated hump reduction rhinoplasty can be done through either an open or closed approach depending on the surgeon’s confidence and experience.
As her results show, a near isolated hump reduction rhinoplasty can be done if other structures of the nose need no to minimal manipulation. For most patients this is not possible since significant hump reduction usually changes how the tip of the nose looks as well as the overall nasal length. Computer imaging will make this need clear before surgery. isolated hump reduction rhinoplasty can be done through either an open or closed approach depending on the surgeon’s confidence and experience.
Case Highlights:
1) One of the most commonly requested rhinoplasty changes is that of the bridge of the nose or the hump area.
2) Reducing a hump on the nose requires reduction of both bone and cartilage in the bridge area.
3) Hump reduction can be done alone in rhinoplasty surgery but requires the shape of the tip and the nasolabial angle to be favorable.
Dr. Barry Eppley
Indianapolis, Indiana