


Background: The frontal bone of the skull makes up the bony forehead. Because of its prominence in the upper third of the face, it is frequently exposed to a variety of traumatic forces. To resist these traumatic forces and protect the underlying brain, the frontal bone is thick and very stout. Mild forces are merely deflected and the injury remains in the soft tissues. With stronger forces the frontal bone will fracture exhibiting a range of injuries from non-displaced fracture lines to actual inward displacement of the bone.
With inward displacement of the bone the frontal lobe of the brain is compressed and decompression is mandatory. Such decompression may consist of bringing the frontal bone segments back out and realigning them or it can involve complete removal of the fractured frontal bone segments. The latter treatment is not as common as the former but severe communition of the bone segments may make removal of the fractured bone segments necessary.
In full thickness frontal bone defects that are treated secondarily there are a variety of reconstructive options. The most contemporary approach is to make custom implant from PEEK, PEKK or HTR from the patient’s 3D CT scan. But that option is not available for everyone which makes alternative reconstruction options necessary.


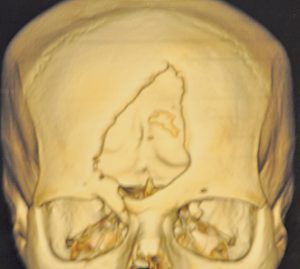 Case Study: This teenage male was involved in a motor vehicle accident in another country which resulted in loss of a central part of the frontal bone and a long vertical forehead laceration/scar. A 3D CT scan showed he extent of the frontal bone defect which involved the frontal sinus.
Case Study: This teenage male was involved in a motor vehicle accident in another country which resulted in loss of a central part of the frontal bone and a long vertical forehead laceration/scar. A 3D CT scan showed he extent of the frontal bone defect which involved the frontal sinus.

 Under general anesthesia and through his existing forehead scar, the frontal bone defect was dissected out freeing the dura from its inner surface and identifying the frontal sinus defect.
Under general anesthesia and through his existing forehead scar, the frontal bone defect was dissected out freeing the dura from its inner surface and identifying the frontal sinus defect.

 The frontal sinus defect was grafted with galea harvested from the inner scalp. A metal mesh was used to create the floor of the frontal bone defect.
The frontal sinus defect was grafted with galea harvested from the inner scalp. A metal mesh was used to create the floor of the frontal bone defect.

 Hydroxyapatite cement was used to cover the mesh and fill it out to the surrounding forehead outer surface. The forehead soft tissue scar was widely excised and the forehead skin closed.
Hydroxyapatite cement was used to cover the mesh and fill it out to the surrounding forehead outer surface. The forehead soft tissue scar was widely excised and the forehead skin closed.

 His 6 month results show a restoration of his forehead contour and a much improved appearance of his forehead scar.
His 6 month results show a restoration of his forehead contour and a much improved appearance of his forehead scar.
There are numerous methods for bony forehead reconstruction. Bone cements are the most historic but they still have a role to play when more contemporary options are not possible. Bone cements, particularly hydroxyapatite cement, need a fir baking when used in full thickness skull defects.
Case Highlights:
1) Restoration of full-thickness forehead bone defects can be done by a variety of techniques, one of which uses hydroxyapatite cement.
2) In full thickness frontal bone defects the frontal sinus must be separated and a strong floor placed onto which the hydroxyapatite cement is placed.
3) In this case surgical access was gained by opening and revising the vertical forehead scar from the initial injury.
Dr. Barry Eppley
Indianapolis, Indiana