

Background: Minor asymmetries of the face are common and are usually more superficial and in the soft tissues. More significant facial asymmetries, however, usually involve the underlying bone. One of the most common areas of significant facial asymmetries involves the lower jaw. Being the only moveable bone on the face and developing from a paired embryonic origin that meets in the middle, it is no surprise that differences between the two formed halves are not uncommon. Since the lower jaw serves as the border between the face and the neck, an asymmetric jaw shape is very evident.
Lower jaw asymmetries present as combinations of horizontal and vertical differences. The chin is almost always involved and deviates either toward one side or is longer or shorter on one side. The jaw angle are usually different in both width and vertical height. More significant jaw asymmetries are not isolated and can also include an occlusal cant indicated that both upper and lower jaws are asymmetric.
The definitive evaluation of lower jaw asymmetries is a 3D CT scan. This provides the complete view of the bony shape of the lower jaw. Provided the occlusion is satisfactory or has a minimal cant to it, the decision on how to correct the jaw asymmetry must take into consideration its external shape. Through computer imaging it can be shown what the aesthetic effects are for various lower jaw changes such as resection of longer side, lengthening of a shorter side and leveling out of the chin.


 Case Study: This middle-aged male presented with a primary vertical lower jaw asymmetry. The right side was too long and the left side was vertically short. The chin was significantly asymmetric in length due to the differences between tow twi sides of the lower jaw. Despite these dramatic differences between the two sides of the lower jaw, his occlusal plane was level.
Case Study: This middle-aged male presented with a primary vertical lower jaw asymmetry. The right side was too long and the left side was vertically short. The chin was significantly asymmetric in length due to the differences between tow twi sides of the lower jaw. Despite these dramatic differences between the two sides of the lower jaw, his occlusal plane was level.
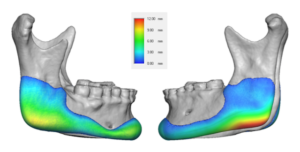
 It was determined by computer imaging that a reduction of the right chin and anterior jawline combined with vertical lengthening of the left side from jaw angle across to the right side of the chin was best. There were limitations as to how much the longer right side due to the lower position of the inferior alveolar nerve in the bone.
It was determined by computer imaging that a reduction of the right chin and anterior jawline combined with vertical lengthening of the left side from jaw angle across to the right side of the chin was best. There were limitations as to how much the longer right side due to the lower position of the inferior alveolar nerve in the bone.
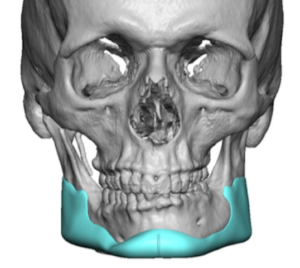
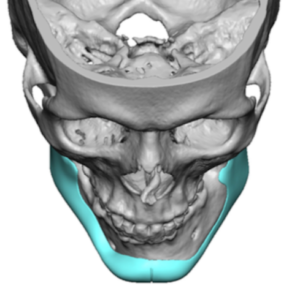
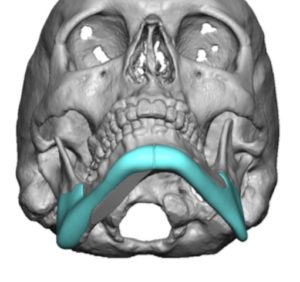
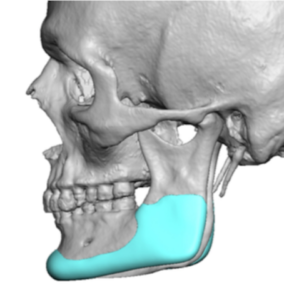 The custom jawline implant design lengthened the left side of the lower jaw and chin and added some width to the entire right side for a more balanced entire lower jaw appearance.
The custom jawline implant design lengthened the left side of the lower jaw and chin and added some width to the entire right side for a more balanced entire lower jaw appearance.

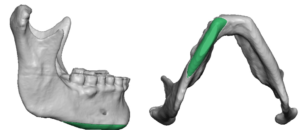
 Under general anesthesia and through a submental incision a right inferior border of 4 to 5mms was done back to the mid-body of the mandible. The bone removed was compared to the custom jawline implant that was yet to be placed.
Under general anesthesia and through a submental incision a right inferior border of 4 to 5mms was done back to the mid-body of the mandible. The bone removed was compared to the custom jawline implant that was yet to be placed.
 Intraoral posterior vestibular incisions were made to create the jaw angle pockets and connect them to the chin. Using a front to back insertion technique the jawline implant was inserted and secured with screws.
Intraoral posterior vestibular incisions were made to create the jaw angle pockets and connect them to the chin. Using a front to back insertion technique the jawline implant was inserted and secured with screws.
 Custom jawline implants can be designed to help with the correction of aesthetic jaw asymmetries by providing length to the shorter wide as well as width if needed to the longer side. This can be combined with bone reduction by ostectomies on the longer side. The vertical reduction on the longer side is limited by the lower intrabony position of the inferior alveolar nerve.
Custom jawline implants can be designed to help with the correction of aesthetic jaw asymmetries by providing length to the shorter wide as well as width if needed to the longer side. This can be combined with bone reduction by ostectomies on the longer side. The vertical reduction on the longer side is limited by the lower intrabony position of the inferior alveolar nerve.
Case Highlights:
1) Significant lower jaw asymmetry exists when the two sides of the mandibles have vertical level differences.
2) Correction of vertical lower jaw asymmetry considers whether one side alone can be treated (augmentation of shorter side or reduction of longer side) or whether both sides must be concurrent treated
3) Many cases of vertical lower jaw asymmetry require a combination of reduction of the longer side and a custom jawline implant for the shorter side to get the best jaw asymmetry correction.
Dr. Barry Eppley
Indianapolis, Indiana