


Background: Hip implants are the newest implant method of augmentative body contouring. Their recent emergence as an aesthetic option for hip augmentation has been generated by the widespread popularity of fat injection buttock augmentation (Brazilian Butt Lift) and the need to have the lateral hip areas complement it as well as the lack of consistent success of fat injection hip augmentation. For thin women, just like in buttock augmentation, hip implants may be the only option due to lack of adequate body fat to harvest.
Hip implants poses several unique challenges compared to all other body implants. To get the correct position for most patients, the implant needs to be placed on top of the TFL fascia (suprafascial pocket) where the risks of postoperative seroma formation is significant. The incisional access to do so is often placed at the bikini line at a location where it can be hidden by clothes but is also at some distance from the inferior extent of the pocket. Also, due to the recent emergence of the use of hip implants no standard implant styles exist and it is not known what the ideal implant shape should be. (thus they are currently made custom for each patient)
Due to the distance between the incision and the desired lowest end of the implant pocket, a highly positioned implant is one of the risks of the surgery. Should this occur the options for repositioning of the implant are challenging. How much it needs to be lowered will influence what type of implant repositioning approach is used.
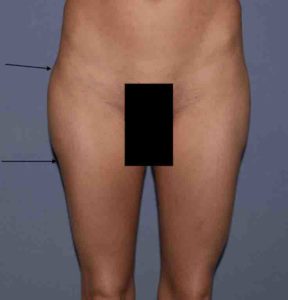

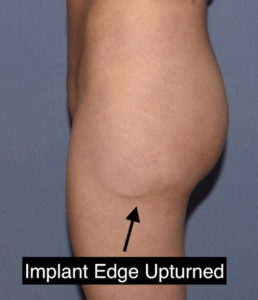 Case Study: This very thin female had a prior history of hip implants placed through a bikini line incision. Due to high positioning and seromas she had a revisional procedure where the implants were attempted to the lowered through her bikini line incisions which was not successful. When I saw her the implants where too high by her desired aesthetic goals as well as she had a slight visible implant edge on the right side and a clearly visible and palpable inferior edge of the implant where it was above the TFL fascia and right up against the skin.
Case Study: This very thin female had a prior history of hip implants placed through a bikini line incision. Due to high positioning and seromas she had a revisional procedure where the implants were attempted to the lowered through her bikini line incisions which was not successful. When I saw her the implants where too high by her desired aesthetic goals as well as she had a slight visible implant edge on the right side and a clearly visible and palpable inferior edge of the implant where it was above the TFL fascia and right up against the skin.

 Given the goal of a 4cm lowering of each implant, lack of success of a prior effort through the high bikini line incision and a malpositioned edge of the left implant it was decided to do a direct approach to the repositioning.
Given the goal of a 4cm lowering of each implant, lack of success of a prior effort through the high bikini line incision and a malpositioned edge of the left implant it was decided to do a direct approach to the repositioning.




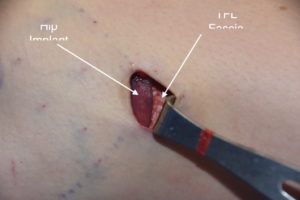
 Under general anesthesia and in the supine position, a 2 cm skin incision was made right at the desired lower end of the new implant position. Once down on the TFL fascia dissection was carried superiorly to the implant capsules. The capsules were opened on each side of the implant up to the widest part of the implant on each side of superiorly. This allowed the implant to drop down where it was secured to the TFL fascia.
Under general anesthesia and in the supine position, a 2 cm skin incision was made right at the desired lower end of the new implant position. Once down on the TFL fascia dissection was carried superiorly to the implant capsules. The capsules were opened on each side of the implant up to the widest part of the implant on each side of superiorly. This allowed the implant to drop down where it was secured to the TFL fascia.
Postoperatively she was advised that the implant could slide back up as there remained the superior part of the pocket, lined with a capsule, which remained present. Circumferential compression wraps were applied to help keep the implant down in its new location as she healed. This is the one time that gravity works in the favor of the implant repositioning effort.
 The best benefit of a direct incision at the desired inferior location of the repositioned hip implant is that it provides the most assured method of visually seeing the implant and getting it into position so that it moves down freely. While the implant is sutured to the TFL fascia the soft silicone quality of the implant does not provide good suture retention so this alone is never adequate to ensure its new inferior position. It is done because it is convenient to do so but the key is adequate capsulotomies and inferior pocket creation.
The best benefit of a direct incision at the desired inferior location of the repositioned hip implant is that it provides the most assured method of visually seeing the implant and getting it into position so that it moves down freely. While the implant is sutured to the TFL fascia the soft silicone quality of the implant does not provide good suture retention so this alone is never adequate to ensure its new inferior position. It is done because it is convenient to do so but the key is adequate capsulotomies and inferior pocket creation.
Case Highlights:
1) Inferior respositioning of high hip implants may be able to be done through the original incision or a new inferior incision is needed.
2) Due to the shape of hip implants capsulotomies need to be performed from the widest part of the implant and down along what lies below it.
3) A direct incision at the desired inferior point with suturing to the TF fascia is the most assured method of stable inferior repostioning in some patients.
Dr. Barry Eppley
Indianapolis, Indiana