

Background: Implants are the assured permanent method of buttock augmentation even though they are far less commonly performed compared to BBL surgery. (fat injections) Patients typically seek out buttock implants because they do not have adequate fat stores to harvest for BBL surgery or they have received inadequate BBL results. The present debate with buttock implants is whether they should be placed on top of or inside the gluteus maximus muscle. (subfascal vs intramuscular) This decision is driven by the size of the buttock increase desired, surgeon preference/experience and the patient’s tolerance for complications.
By far the use of the intramuscular position for buttock implants has fewer potential complications than the subfascial location on the top of the muscle. While it is a far more difficult procedure to create the implant pocket where there is not a natural tissue plane, its deeper position in the buttock tissues is the key for lowering complications. The risks of infection, the development of various types of fluid collections (hematoma, seroma) and shifting of implant position long term after surgery are all lowered by being in a well vascularized and tighter tissue pocket.
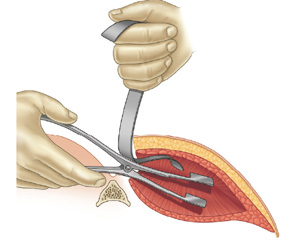 The hardest aspect of intramuscular buttock implant placement is creating the right level of the pocket inside the gluteus maximus muscle. It appears ‘simple’ when looking at a diagram but that belies they challenge that comes from working inside a small 7cm incision. Out of fear of injury to the sciatic nerve the common error is to make the intramuscular pocket too shallow with a thin overlying muscle layer. This usually results in muscle atrophy over the implant and it eventually ends up in a subfascial position. Conversely one does not want to be too deep and traumatize/compress the sciatic nerve. Fortunately the gluteus muscle is quote thick (6 to 8 mms) and creating an intramuscular pocket 2 to 3 cms from the outer surface is at the right level.
The hardest aspect of intramuscular buttock implant placement is creating the right level of the pocket inside the gluteus maximus muscle. It appears ‘simple’ when looking at a diagram but that belies they challenge that comes from working inside a small 7cm incision. Out of fear of injury to the sciatic nerve the common error is to make the intramuscular pocket too shallow with a thin overlying muscle layer. This usually results in muscle atrophy over the implant and it eventually ends up in a subfascial position. Conversely one does not want to be too deep and traumatize/compress the sciatic nerve. Fortunately the gluteus muscle is quote thick (6 to 8 mms) and creating an intramuscular pocket 2 to 3 cms from the outer surface is at the right level.
Case Study: This patient specifically desired intramuscular buttock implants of which the size discussed was in the range of 300 to 400ccs. It was agreed that whatever the size of the implant that could be placed with good muscular closure over it would be used. While maximal implant size was desired, an implant size that fit comfortably in the intramuscular pocket takes precedence.
 Under general anesthesia in the prone position a 7 cm intergluteal incision was made preserving the deeper subcutaneous tissues in the midline. Dissection was carried obliquely once beneath the skin on each side of they midline until the gluteal muscle fascia was encountered. Dissection was carried out on top of the fascia until a god amount of muscle length could be seen. The muscle fibers were then split and blunt dissection carried down until the spinous process of the sacrum was identified. At this level the intramuscular pocket was developed with a variety of blunt dissecting instruments. Implant sizers were placed until the pocket was developed in the range of 350ccs. Using ultrasoft solid silicone buttock implants (330cc natural contour shape), they were inserted with the aid of a funnel device.
Under general anesthesia in the prone position a 7 cm intergluteal incision was made preserving the deeper subcutaneous tissues in the midline. Dissection was carried obliquely once beneath the skin on each side of they midline until the gluteal muscle fascia was encountered. Dissection was carried out on top of the fascia until a god amount of muscle length could be seen. The muscle fibers were then split and blunt dissection carried down until the spinous process of the sacrum was identified. At this level the intramuscular pocket was developed with a variety of blunt dissecting instruments. Implant sizers were placed until the pocket was developed in the range of 350ccs. Using ultrasoft solid silicone buttock implants (330cc natural contour shape), they were inserted with the aid of a funnel device.

 Once in the pocket and with certainty that all implant edges were unfolded, the muscle was closed over the implant. A four layer closure was done over the muscle closure of two fascial layers, dermis and skin. The key in closure, beside the multiple layers, is to recreate the depth of the intergluteal cleft.
Once in the pocket and with certainty that all implant edges were unfolded, the muscle was closed over the implant. A four layer closure was done over the muscle closure of two fascial layers, dermis and skin. The key in closure, beside the multiple layers, is to recreate the depth of the intergluteal cleft.



 Intraoperative results show they change in buttock size and shape from the 330cc intramuscular buttock implants. The depth of the intergluteal cleft has been adequately restored from the closure.
Intraoperative results show they change in buttock size and shape from the 330cc intramuscular buttock implants. The depth of the intergluteal cleft has been adequately restored from the closure.
Case Highlights:
1) Various types of non-female patients undergo buttock enhancement surgery, much less frequently than in females, but with outcomes that are just as successful.
2) The intramuscular buttock implant placement technique is most ideally suited for those patients who prefer an improved shape over a large increase in buttock size.
3) A midline intergluteal incision is preferred for intramuscular buttock implants with emphasis on closure of re-establishing the depth of the intergluteal cleft.
Dr. Barry Eppley
Indianapolis, Indiana