

Background: The two most common midfacial aesthetic deficiencies are undereye hollows and lack of cheek projection. Standard implants have been available for years to to treat these aesthetic midfacial concerns but they often are not adequate. Tear trough implants can improve some undereye deficiencies but it does not provide a complete infraorbital rim augmentation effect. Cheek implants are widely used but their effects are limited to adding volume to the main body of the cheek and submalar area. Putting these two standard implants together can create a combined midfacial augmentation effect but it is not a smooth linear one that resembles a natural bone shape.
The custom infraorbital-malar (IOM) implant creates a high line off augmentation from the undereye area out onto the zygomatic arch in a smooth linear fashion. This is a unique method of midface augmentation that concurrently addresses two problems that are actually related. Undereye hollows that have a skeletal basis are interrelated to lack of cheek projection given that they are developmentally part of the same zygomatico-maxillary bone complex. That interrelationship is best seen in the classic cheekbone/ZMC fracture pattern where the orbit and the cheekbone are seen to be change position together as a combined structure.
In creating many custom infraorbital-malar implants the most difficult design aspect to predict is cheek projection. This specifically refers to where the implant ‘turns the corner’ in the change between the eye area and the side of the cheek. This is also the area of the Ogee curve. It is the most aesthetically sensitive and can make the difference between an aesthetically pleasing outcome or one in which it looks too big. As a result I tell all patients I reserve the right to modify the size of the implant should I feel it looks too big in this area of the implant during surgery
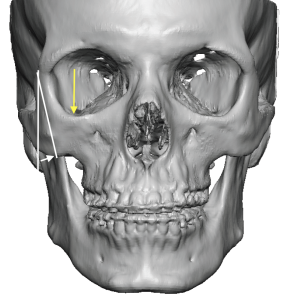
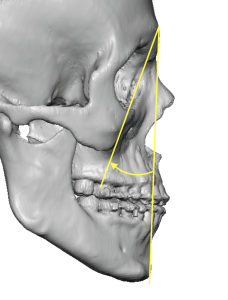 Case Study: This male desired a modest undereye and high cheekbone look. His 3D CT scan showed some of the classic findings seen in undereye hollows (dip in lateral infraorbital rim – yellow arrow) and inward angulation of the cheekbone. (white angles)
Case Study: This male desired a modest undereye and high cheekbone look. His 3D CT scan showed some of the classic findings seen in undereye hollows (dip in lateral infraorbital rim – yellow arrow) and inward angulation of the cheekbone. (white angles)
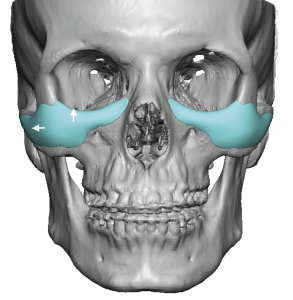
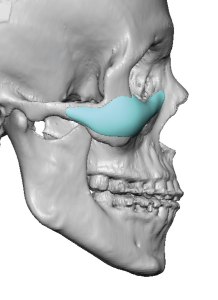 Custom infraorbital-malar implants were designed to add vertical infraorbital rim height with saddling, a high cheekbone effect with extension out onto the zygomatic arch and a subtle addition to the Ogee curve.
Custom infraorbital-malar implants were designed to add vertical infraorbital rim height with saddling, a high cheekbone effect with extension out onto the zygomatic arch and a subtle addition to the Ogee curve.
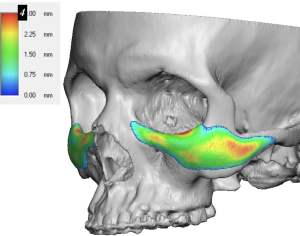
 The maximum implant projection at the ‘curve’ was 4mms, extending a bit out onto the cheekbone proper. Following the line of faint red color it is this high horizontal line that creates the high cheekbone look.
The maximum implant projection at the ‘curve’ was 4mms, extending a bit out onto the cheekbone proper. Following the line of faint red color it is this high horizontal line that creates the high cheekbone look.
 During surgical implantation through a limited lower eyelid incision, I felt that its effect on the cheek and arch was too strong. This made his cheeks look too wide. This the implants were modified on the back table to create a less strong and more subtle augmentation in this area.
During surgical implantation through a limited lower eyelid incision, I felt that its effect on the cheek and arch was too strong. This made his cheeks look too wide. This the implants were modified on the back table to create a less strong and more subtle augmentation in this area.

 The effects of the modified IOM implants could be seen in the front view.
The effects of the modified IOM implants could be seen in the front view.
While its is often said that a millimeter or two on the face makes a big difference…that is largely not true. The exception where it is true is in the cheek area where the soft tissues are thin and it is in a highly seen area due to the location of the adjacent eyes. As a result, about half of all IOM implants I do receive an intraop reduction in the curve areas of the implants to avoid an overcorrection and an unnatural look. It is also why I don’t usually make an IOm implant more than 4mms in this area unless the patient has a significant infraorbital-malar deficiency that is associated with a negative orbital vector.
Case Highlights:
1) Undereye and cheeks deficiencies can be seen on 3D CT scans by an abnormality in the infraorbital rim shape and the inward angulation of the cheekbone.
2) The connected infraorbital-malar implant improves undereye hollows and cheek-arch projection in a single implant design.
3) It is not uncommon that custom infraorbital-malar implants are modified in surgery due to excessive cheek width and arch prominence.
Dr. Barry Eppley
Indianapolis, Indiana