

Background: Cheek implants are the most common surgical method of midface augmentation. But determining what the shape and amount that the cheek augmentation should be for any particular patient is far from an exact science. Unlike chin implants, in which linear assessment and computer imaging can really help define what the patient wants to achieve, the shape and size of the cheeks can not so easily be assessed. There are also aesthetic gender differences in the cheeks that are also as significant, if not more so, than in chin augmentation.
While some women like the apple cheek fullness look (low anterior fullness) men absolutely do not. That would be considered a feminizing effect. Men prefer a highlighted bone appearance to their midface often referred to as the high cheekbone look. This is a more linear midface appearance that places the volume along the infraorbital-malar bony line. In some ways this is the companion to the linear effect of jawline augmentation. Where the volume is distributed along this bony line is a matter of patient preference. Such a high cheekbone look can not be achieved by the use of standard cheek implants to date.
Currently only custom cheek implant designs can achieve the midface look that many men and some women desire. In designing this type of cheek implant the key question is what should the volume/thickness be in turning the curve around the main body of the cheekbone. It is easy to over estimate the volumetric effect of augmenting this midface area particularly when the implant is completely over the bone. This is an area that during the custom cheek implant placement the surgeon needs to be prepared to modify the implant if needed if it looks too large.
Case Study: This male wanted cheek augmentation and was very specific about the look he desired. Like many patient sh showed numerous examples of the type of cheek look he sought using celebrity pictures as examples. He did not specifically request any undereye augmentation.
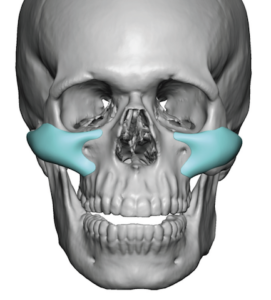
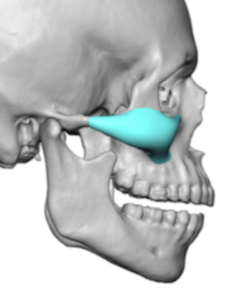
 In designing this type of male cheek implant it is first important to determine the path of insertion which in this case would be intraoral. (since there is no significant intrafraorbital component to it) The footprint of the implant covers the entire zygomatic body and arch. To help with the intraoral placement and positioning of the implant a maxillary extension is added as part of the design.
In designing this type of male cheek implant it is first important to determine the path of insertion which in this case would be intraoral. (since there is no significant intrafraorbital component to it) The footprint of the implant covers the entire zygomatic body and arch. To help with the intraoral placement and positioning of the implant a maxillary extension is added as part of the design.
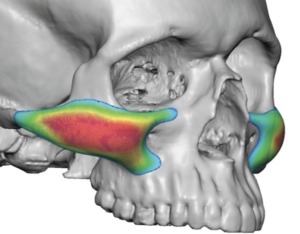
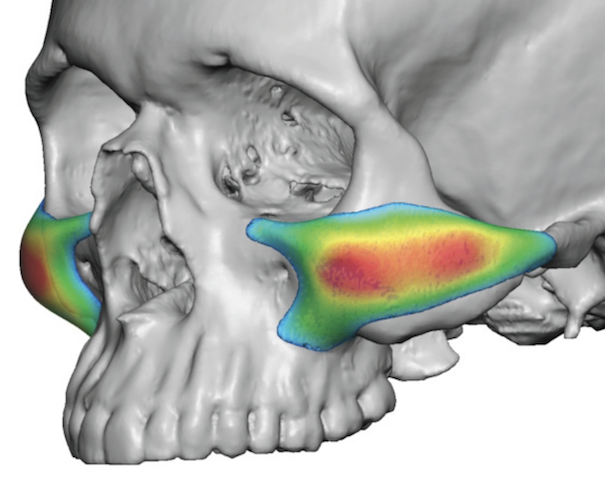
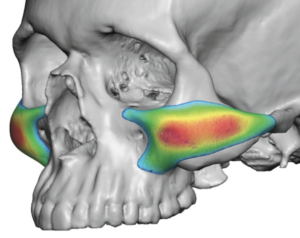 The most thoughtful part of the design, and of great importance, is the thickness of the implant across the zygomatic body and arch. As a general guideline I don’t like to make the thickness around the implant as it turns the curve more than 4mms. It would be very rare that anyone needs more than that and often even that amount can be too much unless one has a significant infraorbital-skeletal deficiency. To ensure that the shape/thickness of the implant creates a high linear look the color mapping of the implant thicknesses is very helpful.
The most thoughtful part of the design, and of great importance, is the thickness of the implant across the zygomatic body and arch. As a general guideline I don’t like to make the thickness around the implant as it turns the curve more than 4mms. It would be very rare that anyone needs more than that and often even that amount can be too much unless one has a significant infraorbital-skeletal deficiency. To ensure that the shape/thickness of the implant creates a high linear look the color mapping of the implant thicknesses is very helpful.

 The custom cheek implants were placed through a high vestibular incision over the posterior maxilla. In looking at them the prominent of the cheek curve seemed too strong. Using a #10 scalp blade its prominence was reduced to a less round curve.
The custom cheek implants were placed through a high vestibular incision over the posterior maxilla. In looking at them the prominent of the cheek curve seemed too strong. Using a #10 scalp blade its prominence was reduced to a less round curve.
 Once reinserted a single small screw was used to secure the implant to the zygomatic buttress. The low end of the maxillary extension was then removed to keep any implant edge away from the incisional closure.
Once reinserted a single small screw was used to secure the implant to the zygomatic buttress. The low end of the maxillary extension was then removed to keep any implant edge away from the incisional closure.
In the design of custom cheek implants it is impossible to know to any high degree of accuracy what their aesthetic effects will be. I have seen many more custom cheek implant patients that felt their prominence was too much than those who felt it was not enough. Thus it is prudent to consider reducing the strength of the curve if it looks like it sticks out unnaturally. While the patient is not awake to assist in this intraoperative decision it usually proves to be the correct one.
Case Highlights:
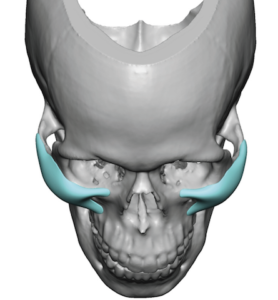
1) Cheek implants in men should generally follow the horizontal line of bone from below the eye back across the cheeks to create the high cheekbone look.
2) In custom designing cheek implants the most common preoperative unknown is how much augmentation is too much around the curve.
3) Intraoperative reduction of custom cheek implants is not uncommon when they appear too prominent during surgery.
Dr. Barry Eppley
Indianapolis, Indiana