

Background: Chin implants can be inserted from either an external or intraoral approach. There are advantages and disadvantages with either approach and both can be equally successful with good surgical technique. While the intraoral approach is scarless it is prone to somewhat higher risks of malposition (superiorly) and infection. The most common of the two is malposition which almost universally is associated with a lack of implant screw fixation. Without a method to hold the implant down it is inevitable that it will quickly slide upwards toward the incision.
When replacing a chin implant with a custom jawline implant, regardless of the method by which the chin implant was placed, the anterior approach is usually done externally. (submental incision) I advocate this incisional approach in an effort to lower the infection risk by lowering implant exposure to mouth bacteria, Most men do not object to the submental incision but occasionally some do. As long as they understand the increased infectivity risk a custom jawline implant can be inserted through three intraoral incisions of it is not overly large.

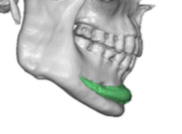 Case Study: This Asian male had a history of a prior chin implant which never made much of a difference and was now interested in a more complete jawline augmentation effect. The 3D CT scan needed for the custom jawline implant showed a very highly positioned implant that had virtually no effect on increasing the horizontal chin projection.
Case Study: This Asian male had a history of a prior chin implant which never made much of a difference and was now interested in a more complete jawline augmentation effect. The 3D CT scan needed for the custom jawline implant showed a very highly positioned implant that had virtually no effect on increasing the horizontal chin projection.
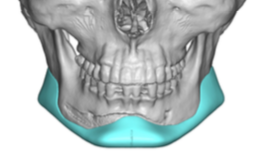
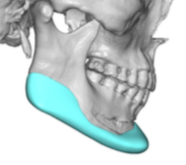 The custom jawline implant design developed provided definite greater horizontal chin projection and an entire jawline effect behind it.
The custom jawline implant design developed provided definite greater horizontal chin projection and an entire jawline effect behind it.
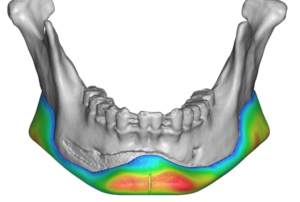
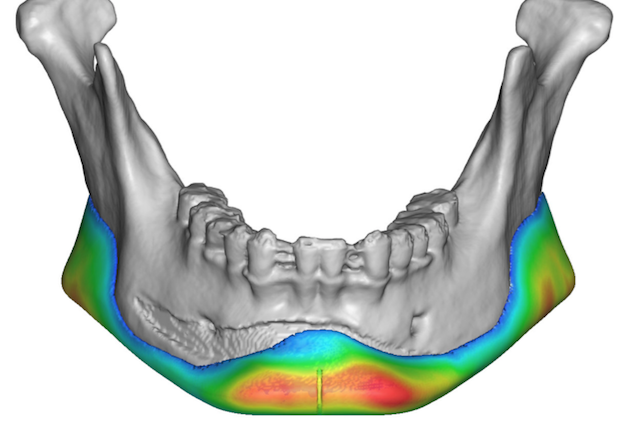
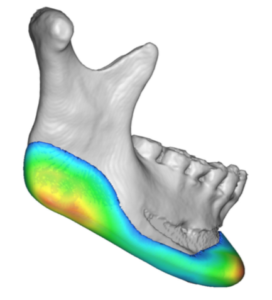 Closer inspection of the scan shows limited implant bone imprinting at the level above the jawline implant design.
Closer inspection of the scan shows limited implant bone imprinting at the level above the jawline implant design.

 The patient desired on having the procedure performed completely inside the mouth. Initially the previous intraoral vestibular incision was opened to expose the existing chin implant. On its removal four large spikes of bone could be seen that had grown up through the holes in the chin implant.
The patient desired on having the procedure performed completely inside the mouth. Initially the previous intraoral vestibular incision was opened to expose the existing chin implant. On its removal four large spikes of bone could be seen that had grown up through the holes in the chin implant.

 These bone ingrowths were removed as well as the entire capsule on the bone so that the subperiosteal implant pocket could be created back to the jaw angles. The jawline implant was successfully inserted through the anterior vestibular incision as one piece in a front to back insertion fashion. Three screws were inserted in the chin portion of the implant and one screw at each jaw angle implant.
These bone ingrowths were removed as well as the entire capsule on the bone so that the subperiosteal implant pocket could be created back to the jaw angles. The jawline implant was successfully inserted through the anterior vestibular incision as one piece in a front to back insertion fashion. Three screws were inserted in the chin portion of the implant and one screw at each jaw angle implant.
Case Highlights:
1) Superior chin implant displacement is common when an intraoral insertion method is used.
2) Chin implants show a classic imprinting pattern on the bone and sometimes bone ingrowth up through the holes of the implant.
3) Intraoral placement of custom jawline implants can be done in men but are associated with a higher risk of infection.
Dr. Barry Eppley
Indianapolis, Indiana