

Background: Augmentation of the periorbital region has very few standard implant options. Such standard implants are made for the aesthetic tear trough deformity and some modest amount of horizontal infraorbital rim deficiency. Combined with cheek implants an infraorbital-malar horizontal augmentation can be achieved but not in a contiguous fashion.
But specific types of infraorbital-malar augmentations can only be achieved by a custom design approach. When the infraorbital rim augmentation requires a vertical component and needs to saddle the rim and/or when the cheek augmentation must remain high and far out onto the zygomatic arch (high cheekbone look), these are not bony augmentations that can be achieved with any type of standard implant shape or material.
When you look at aesthetic infraorbital-malar deficiencies the entire zygomatic-orbital complex is underdeveloped. The cheekbone and zygomatic arch is tilted inward as well as that of the infra- and lateral orbital rims. The finding is that the infra- and lateral orbital rim is low as well. The infraorbital rim sits well below the lower eyelid and the lower eyelid fat pads will show. (pseudoherniation) Augmenting this midface deficiency requires a topographically complex design as a single implant.
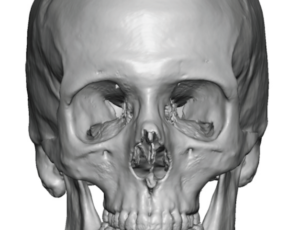
 Case Study: This male had flat cheeks, deep undereye hollows and pseudoherniated fat. His 3D CT scan showed infraorbital rim asymmetry (right lower than left) and lack of any convexity to the zygomatic arches.
Case Study: This male had flat cheeks, deep undereye hollows and pseudoherniated fat. His 3D CT scan showed infraorbital rim asymmetry (right lower than left) and lack of any convexity to the zygomatic arches.
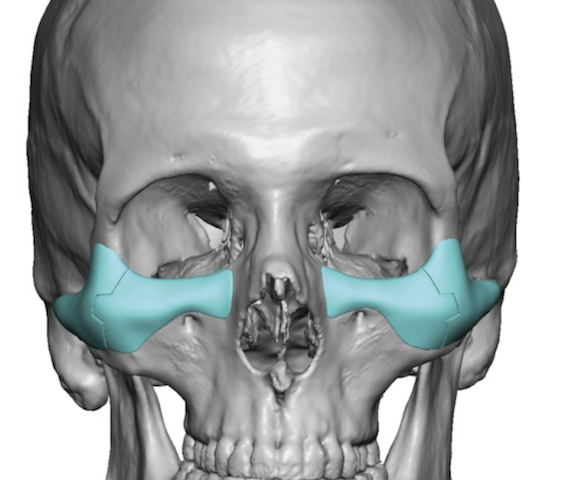
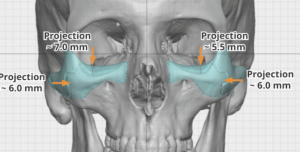 Custom infraorbital-malar implants were designed to build out the entire area from the edge of the nasal bones medially all the way out to the end of the zygomatic arch. The infraorbital rims were elevated significantly (7/5.5) and the cheek projection was significant. (6mms) Geometric split lines were marked into the design in case the implants had to be separated to be placed. (which did not turn out to be necessary)
Custom infraorbital-malar implants were designed to build out the entire area from the edge of the nasal bones medially all the way out to the end of the zygomatic arch. The infraorbital rims were elevated significantly (7/5.5) and the cheek projection was significant. (6mms) Geometric split lines were marked into the design in case the implants had to be separated to be placed. (which did not turn out to be necessary)
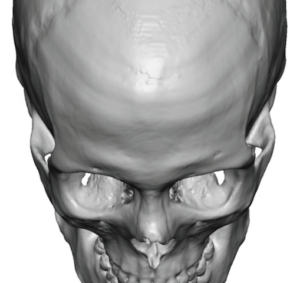
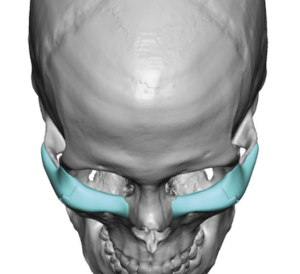
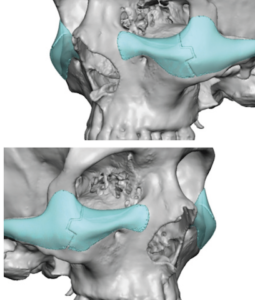 In the spirit of a ensuring a high cheekbone look in a male, the oblique views showed the location of the projection/curve of the cheeks.
In the spirit of a ensuring a high cheekbone look in a male, the oblique views showed the location of the projection/curve of the cheeks.
 Under general anesthesia and through lower eyelid incisions, the subperiosteal pockets were created and the implants placed as a single piece.
Under general anesthesia and through lower eyelid incisions, the subperiosteal pockets were created and the implants placed as a single piece.

 Microscrew fixation was used on each side. The cheek tissues were resuspended up over the implants and lateral canthopexies performed.
Microscrew fixation was used on each side. The cheek tissues were resuspended up over the implants and lateral canthopexies performed.
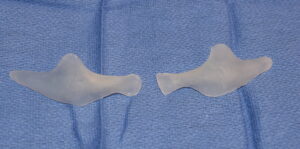
Custom infraorbital-malar implants of this size and dimensions would be considered large and unsuitable for most patients. But when a skeletal deficiency exists in a larger fuller face it really takes this much volume to make a visible difference. The implants certainly didn’t look too big for him and and his face ‘swallowed up’ more of the implant volume that one would think could happen. Meaning that although these were large implants they ended up looking natural like they belonged there.
Case Highlights:
1) Most significant infraorbital-malar bony deficiencies have vertical rim deficiency often with asymmetry between the two sides.
2) A custom infraorbital-malar implant design is the only method to contiguously and smoothly expand the lower orbital and cheek bone boundaries.
3) A transcutaneous lower eyelid incision offers the direct access needed for the subperiosteal dissection and placement of this large midface implant that saddles the infraorbital rim.
Dr. Barry Eppley
Indianapolis, Indiana