


Background: The sliding genioplasty is the autologous option for chin augmentation that has both its advocates and advantages in the properly selected patient. In the ‘average’ chin augmentation patient, where horizontal augmentation is the need, it completes with chin implants and the decision between the two must be carefully considered by the patient.
When the chin augmentation needs becomes larger (10mms or greater of horizontal projection ) the use of chin implants become very limited unless custom designs are used. Implants become more limited at these amounts of augmentation due to lack of available sizes that provide that much augmentation and the ability of the soft tissue chin pad to stretch over it.
The role of a sliding genioplasty becomes more unequivocal at these larger horizontal movements. The attached soft tissues to the bone negates any issues of chin pad stretch and the internal attached muscles to the back side of the chin bone have good ability to stretch. The intraoperative issues to consider are adequate bone stabilization and ensuring that bone healing will occur more limited bbne contact between the upper and lower chin segments.
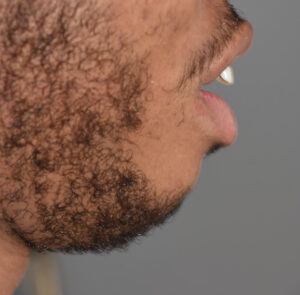
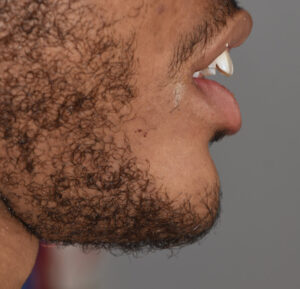
Case Study: This male had a large chin deficiency which was almost 20mm in horizontal deficiency. He had a short lower jaw but orthognathic surgery was not an option he wanted to pursue. He had a very round chin shape in side profile.
 sliding genioplasty dr barry eppley IndianapolisUnder general anesthesia and through an intraoral approach a low angled osteotomy cut was made through the chin below the mental nerve exits and sufficiently behind it. Once downfractured the chin bone was advanced 16mms and a plate and screws used to stabilize it.
sliding genioplasty dr barry eppley IndianapolisUnder general anesthesia and through an intraoral approach a low angled osteotomy cut was made through the chin below the mental nerve exits and sufficiently behind it. Once downfractured the chin bone was advanced 16mms and a plate and screws used to stabilize it.

 The bone gap created by the advancement was initially grafted by an allergenic bone block. The long bone block was sectioned into pieces to place on both sides of the plate in the bone gap. It was initially soaked in an antibiotic-betadine solution.
The bone gap created by the advancement was initially grafted by an allergenic bone block. The long bone block was sectioned into pieces to place on both sides of the plate in the bone gap. It was initially soaked in an antibiotic-betadine solution.

 Allogeneic bone chips were then placed between the bone block and into all remaining bone gaps to completely cover the plate as well. It was prepared by initially being wetted with antibiotic powder and saline.
Allogeneic bone chips were then placed between the bone block and into all remaining bone gaps to completely cover the plate as well. It was prepared by initially being wetted with antibiotic powder and saline.
 Once grafted a two layer muscle and final mucosal layer was done for closure. HIs immediate intraop result laying on the operating table was impressive as would be expected with such a bony chin movement.
Once grafted a two layer muscle and final mucosal layer was done for closure. HIs immediate intraop result laying on the operating table was impressive as would be expected with such a bony chin movement.
The bone gap created by large sliding genioplasties should ideally be grafted with autologous bone from the patient. But that is not too appealing to the patient for understandable reasons. Thus allogeneic or tissue back bone is used which is the second best option.
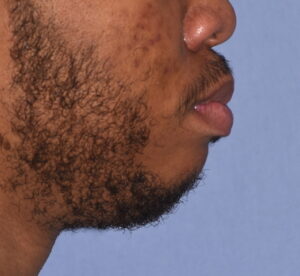



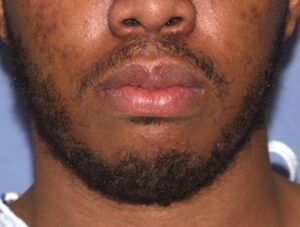
 When seen one day after surgery this patient had a very noticeable improvement in his facial proportions. While he initially presented for total jawline augmentation this chin augmentation result alone is likely to be adequate for him.
When seen one day after surgery this patient had a very noticeable improvement in his facial proportions. While he initially presented for total jawline augmentation this chin augmentation result alone is likely to be adequate for him.
Case Highlights:
1) Large sliding genioplasties would be considered any forward movement of 10mms or greater.
2) Large movement sliding genioplasties may result in limited bony contact to the lateral wing areas.
3) Bacause of #2 bone grafting is needed of which allogeneic block or corticocancellous chips are acceptable.
Dr. Barry Eppley
Indianapolis, Indiana