


Background: In chin augmentation the surgical choices are always between an implant and a bony movement of the chin. Patients may have their preference based on their affinity for an autologous procedure (sliding genioplasty) or a less invasive approach (implant), but that decision is overridden when the dimensional changes desired reach a certain point. As a general guideline in a primary chin augmentation when the horizontal changes exceed 10mms and/or the vertical change needed its 7mms or more, either individually and particularly when combined, the sliding genioplasty procedure is needed.
The original sliding genioplasty was indeed a bone slide. The bone was moved forward along the line of the cut and had to stay there because wire fixation was used. It was limited to a maximum movement of whatever distance was achieved when the lingual cortex of the downfractured bone was wired against the buccal cortex of the fixed bone above it. And vertical lengthening changes required an interpositional bone graft. In other words there wasn’t much precision in the dimensional control of the chin augmentation change.
But once plate and screw fixation became available the ability to control where the down fractured chin bone segment was placed changed dramatically. But what is often not appreciated is that with plate and screw fixation is most cases it is no longer a sliding geniopasty. The cut chin bone is moved away from the upper chin segment at least centrally in most cases. The only part of the moved chin bone that touches the bone above it is at the sides. In more dramatic movements only the very back ends of the sides touch. In essence plate and screw fixation in bony genioplasties allows the chin bone to be suspended out into space. The bone survives because of its soft tissue attachments but the bone gap creates between the two bone segments or the size of the step off should be considered for management in the procedure.,
Case Study: This male had a congenitally short chin both horizontally as well as vertically. Preoperative computer imaging looked at a variety of horizontal increases and it was decided that 14mms was needed. But there was also a need for some vertical lengthening. The amount was determined by a habit he did in which he jutted his jaw down and forward . Given that jaw jutting definitely adds vertical lengthening more than a few millimeters was needed.


 Under general anesthesia a bony genioplasty was performed with 14mm forward and 7mms vertical lengthening. Corticocancellous bone blocks were cut and placed into the interpositional gaps. A 3 layer closure was done. (2 muscle layers and an external mucosal layer)
Under general anesthesia a bony genioplasty was performed with 14mm forward and 7mms vertical lengthening. Corticocancellous bone blocks were cut and placed into the interpositional gaps. A 3 layer closure was done. (2 muscle layers and an external mucosal layer)

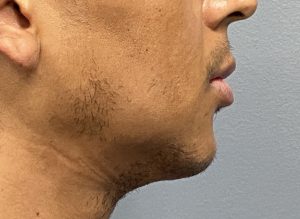

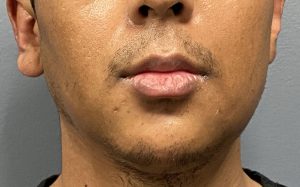 His one day before and after pictures show the tremendous change that only a bony genioplasty could do for him.
His one day before and after pictures show the tremendous change that only a bony genioplasty could do for him.
Most bony geniplasies are more modest in change than this case and are usually under 10mms with limited vertical change. But as the dimensional changes become greater so does the interpositional gap between the two bone segments. To aid a more complete bony consolidation interpositional grafts from a tissue bank source are beneficial.
Case Highlights:
1) One of the advantages of a sliding genioplasty is that it can create both horizontal and vertical dimensional changes that exceed what an implant can do.
2) In large dimensional changes with a sliding genioplasty most of the mobilized bone segment loses contact with the fixed bone above it….thus the need for interpositional bone grafting.
3) The advantages of plate and screw fixation in sliding genioplasties is the ability to control the dimensional changes by plate selection and plate bending.
Dr. Barry Eppley
Indianapolis, Indiana