

Background: Augmentation of the lower third of the face frequently involves placing an implant at the jaw angle area. Whether done as an isolated jaw angle implant or part of an overall custom jawline implant placement of the implant involves knowledge and manipulation of the masseter muscles. This is distinctly different than that of chin augmentation in which the mentalis muscle is neither a limiting factor in implant placement and has a much lower risk of an postoperative problems. (particularly if done from a submental approach)
Proper management of the masseter muscle is the key in any form of jaw angle implant surgery. This is not only relevant to get the implant in the proper position but to prevent undesired retraction of the muscle over the implant after surgery. (masseteric muscle dehiscence. Technically it is not the muscle per se that poses the issue bit its ligamentous attachments at the gonial angle point and alone the inferior border. These ligamentous attachments must be elevated off of the bone particularly if there is any vertical lengthening effect of the implant.
 The ease or difficulty of elevating the ligamentous attachments of the masseter muscle can be seen in a preop 3D CT scan. (which is always needed in custom jawline implants) Strong ligamentous attachments can be seen at the jaw angles as spikes or discrete small mounds of bone along the inferior border often with a more pronounced antegonial notch. Less strong ligamentous attachments will show very small or no bony prominences at all. These bony changes at the jaw angles are a reflection of the old biologic adage of ‘form follows function’. Interestingly and also biologic is that men more often will have CT evidence of these jaw angle bony prominences that most women do not have. Men, of course, usually have larger and stronger masseter muscles hence the anatomic differences from females seen at the bony jaw angles.
The ease or difficulty of elevating the ligamentous attachments of the masseter muscle can be seen in a preop 3D CT scan. (which is always needed in custom jawline implants) Strong ligamentous attachments can be seen at the jaw angles as spikes or discrete small mounds of bone along the inferior border often with a more pronounced antegonial notch. Less strong ligamentous attachments will show very small or no bony prominences at all. These bony changes at the jaw angles are a reflection of the old biologic adage of ‘form follows function’. Interestingly and also biologic is that men more often will have CT evidence of these jaw angle bony prominences that most women do not have. Men, of course, usually have larger and stronger masseter muscles hence the anatomic differences from females seen at the bony jaw angles.

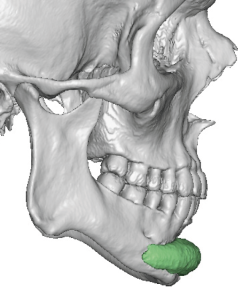
 Case Study: This female desired a jawline augmentation. Her preoperative 3D CT scan showed high jaw angles with fairly smooth inferior borders with only small bony prominences…not completely smooth but close.
Case Study: This female desired a jawline augmentation. Her preoperative 3D CT scan showed high jaw angles with fairly smooth inferior borders with only small bony prominences…not completely smooth but close.
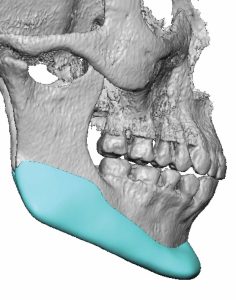
 A custom jawline implant was designed which had 7mms of vertical lengthening which was going to necessitate elevation/release of the muscle ligamentous attachments.
A custom jawline implant was designed which had 7mms of vertical lengthening which was going to necessitate elevation/release of the muscle ligamentous attachments.

 Under general anesthesia and through an external submental skin incision and two intraoral posterior vestibular incisions an inferolateral subperiosteal pocket was elevated with inferior border elevation all the way back through the jaw angles. As the preop scan indicated the inferior border attachments elevated easily without disruption/detachment of the masseter muscle.
Under general anesthesia and through an external submental skin incision and two intraoral posterior vestibular incisions an inferolateral subperiosteal pocket was elevated with inferior border elevation all the way back through the jaw angles. As the preop scan indicated the inferior border attachments elevated easily without disruption/detachment of the masseter muscle.
While fewer females get jaw angle and custom jawline implants they consistently had less rigid ligamentous attachments and easier pocket dissection from men.The preoperative 3D CT scan consistently shows how challenging this ligamentous release will be and the risk of postoperative masseteric muscle dehiscence.
Highlights:
- Vertical jaw angle lengthening is more commonly done in females than in men.
- The anatomy of the female jaw angles is different than in men with less strong masseter muscle attachments as can be evidenced in 3D CT scans.
- Female jaw angle dissections are easier than in men with less risk of postoperative masseteric muscle dehiscence.
Dr. Barry Eppley
World-Renowned Plastic Surgeon